Case presentation
Fetal echocardiography was performed to monitor the fetus of a healthy mother due to increased nuchal translucency at 12 + 2 weeks of gestation. Chorionic villous sampling revealed normal male karyotype. Findings at 19 + 1 weeks included bilateral superior caval veins with the left draining to the coronary sinus, moderate holosystolic tricuspid regurgitation, and pulmonary/aortic valve ratio of 0.68 (lower limit of normal).Reference Beattie, Peyvandi, Ganesan and Moon-Grady 1 The pulmonary to aortic valve ratio was unchanged at 31 + 1 weeks. Isthmic diameter was marginally small for gestational age. The patient was delivered at 38 + 2 weeks. On the first day of life, he became tachypnoeic. A soft systolic murmur was noted. Transthoracic echocardiography verified the presence of bilateral superior caval veins, dilated coronary sinus, and functionally bicuspid aortic valve. Transverse arch diameter was 4 mm. Isthmus was 3 mm. The myocardium of the left ventricle showed prominent trabeculations and deep intertrabecular recesses with impaired contractility (fractional shortening = 24%) and ventricular dilatation. These findings were compatible with left ventricular non-compaction (hereinafter referred to as “noncompaction”) cardiomyopathy. The patient was started on Prostaglandin E2, dopamine, and furosemide. Surgical correction of coarctation was performed on the 4th day of life. Post-operatively captopril and furosemide were started. Fractional shortening of the left ventricle gradually increased to 34%.
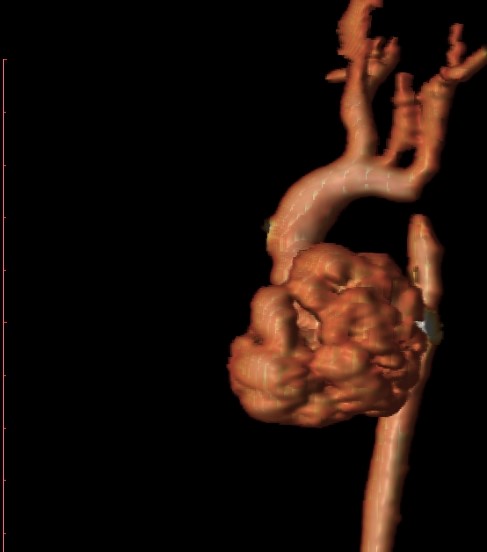
At 3 months of age, the patient showed signs of heart failure. Treatment was modified to captopril, carvedilol, furosemide, and spironolactone. Cardiac MRI showed a spherical left ventricle with moderate wall hypokinesia and an ejection fraction of 43%. There were thin trabeculations and deep intertrabecular recesses compatible with non-compaction (Fig 1a). The trabeculations showed moderate contractility and the ratio of non-compacted/compacted myocardium was >3. There was also significant discrete stenosis of the isthmus just distal to the origin of the left subclavian artery (Fig 1b and c and Supplementary figure S1). The isthmic lumen diameter measured 2.6 mm and the post-stenotic diameter of the thoracic aorta was 5.5 mm. Transverse arch appeared normal. Balloon angioplasty successfully relieved the recoarctation.

Figure 1. ( a ) Left ventricular non-compaction: cardiac MRI shows thin trabeculations and deep intertrabecular recesses. ( b and c ) Discrete stenosis of the aortic isthmus just distal to the origin of the left subclavian artery as shown in cardiac MRI. Bright blood with steady-state precession ( b ). Black blood ( c ).
Three months after catheterisation, fractional shortening was 26%. Diuretics were discontinued due to electrolytic abnormalities. Carvedilol and captopril were maintained. Fractional shortening improved further to 31–33% within the following months. The free wall of the left ventricle and the upper part of the interventricular septum gradually became hypertrophic. A hypertensive trend was controlled with updosing of carvedilol and captopril.
The patient is currently 3 years old, growing well, and remains asymptomatic with an unremarkable physical examination. Left ventricular fractional shortening is maintained at 30–33% and blood pressure is normal.
Discussion
Non-compaction is a heterogeneous myocardial abnormality of unknown aetiology.Reference Anderson, Jensen and Mohun 2 Features include multiple prominent ventricular trabeculations, deep intertrabecular recesses, and a bi-layered myocardium consisting of a thick, spongy, non-compacted endocardial layer and a thin, compacted, epicardial layer.Reference Finsterer, Stollberger and Towbin 3 Abnormal trabeculations are typically most evident in the apical portion of the left ventricle with extension to the lateral left ventricular wall, distal to the papillary muscles.Reference Finsterer, Stollberger and Towbin 3 , Reference Towbin, Lorts and Jefferies 4 The left ventricular cavity communicates with the intertrabecular spaces without evidence of perfusion by the epicardial coronary artery system.Reference Towbin, Lorts and Jefferies 4
It has been speculated that arrest of endomyocardial morphogenesis with failure in the compaction pathway represents the pathogenetic mechanism underlying non-compaction; however, this hypothesis is unproven.Reference Towbin, Lorts and Jefferies 4 It seems more likely that non-compaction of the ventricular myocardium results from abnormal persistence of the trabecular layer rather than from non-compaction of the ventricular wall.Reference Henderson and Anderson 5 Indeed, if persistence of the embryonic sinusoids was the pathogenetic mechanism, direct communication with the coronary arteries would be expected and should have been documented; however, this contradicts the definition of non-compaction.Reference Finsterer, Stollberger and Towbin 3 , Reference Towbin, Lorts and Jefferies 4 Also, as the excessive trabeculations in non-compaction lack embryonic features (sparse Purkinje cells, atrial natriuretic factor negative, and abundant in coronary vasculature), non-compaction cannot be considered a retention of the embryonic design. Therefore, the lesion may result from the compact wall growing into the ventricular lumen in a trabecular fashion.Reference Jensen, van der Wal, Moorman and Christoffels 6 Indeed, antenatal echocardiograms did not identify foetal non-compaction in our patient.
Non-compaction was originally reported as an isolated cardiomyopathy.Reference Finsterer, Stollberger and Towbin 3 , Reference Towbin, Lorts and Jefferies 4 However, non-compaction has been subsequently described in all age groups in association with most forms of CHD. Right-sided lesions, especially Ebstein’s anomaly, pulmonic stenosis, pulmonary atresia, tricuspid atresia, and tetralogy of Fallot, are more frequently coupled with non-compaction. Congenital non-compaction has been associated with distinct genetic mutations, albeit a causal relationship between these monogenic disorders and non-compaction remains to be established.Reference Finsterer, Stollberger and Towbin 3 Genetic abnormalities may cause both structural malformations and impair left ventricular myocardial differentiation. Haemodynamic disturbances during foetal life or post-natally may trigger or contribute to alterations of left ventricular architecture in genetically susceptible individuals.Reference Finsterer, Stollberger and Towbin 3 , Reference Stahli, Gebhard and Biaggi 7
Cardiac magnetic resonanceReference Secchi, Di Leo and Papini 8 criteria for the diagnosis of non-compaction includeReference Nucifora, Sree Raman and Muser 9 : visual appearance of two distinct myocardial layers (a compacted epicardial layer and a non-compacted endocardial layer); marked trabeculation and deep intertrabecular recesses within the non-compacted layer; and non-compacted to compacted end-diastolic myocardial ratio >2.3 and/or non-compacted to global end-diastolic left ventricle mass ratio >0.20.
CHD and non-compaction are mainly seen in children.Reference Tsai, Ebenroth, Hurwitz, Cordes, Schamberger and Batra 10 , Reference Yu, Wang, Zheng and Zou 11 The efficacy of surgical treatment of these patients is largely unknown. There is evidence suggesting that the presence of non-compaction may increase the risk of operative repair of congenital cardiac malformations.Reference Tsai, Ebenroth, Hurwitz, Cordes, Schamberger and Batra 10 , Reference Yu, Wang, Zheng and Zou 11 Indeed, children who present with heart failure and poor ventricular function may have worse outcomes (death or intractable heart failure) post-operatively.Reference Yu, Wang, Zheng and Zou 11 In these patients, poor ventricular function may be attributed to non-compaction, CHD, or both. Surgery can effectively relieve heart failure, improve ventricular function, and decrease heart size.Reference Yu, Wang, Zheng and Zou 11 This was the case in our patient, whose left ventricular function was restored post-surgery and balloon angioplasty.
CHD co-exists with non-compaction in 12% of adult cases. The prevalence of non-compaction is highest for Ebstein’s anomaly followed by aortic coarctation, tetralogy of Fallot, and bicuspid or unicuspid aortic valve.Reference Stahli, Gebhard and Biaggi 7 Recent data suggest that bicuspid aortic valve is present in 11% of non-compaction cases.Reference Stahli, Gebhard and Biaggi 7 , Reference Agarwal, Khandheria, Paterick, Treiber, Bush and Tajik 12 , Reference Towbin 13 Notably, only 10 cases of non-compaction with bicuspid aortic valve and coarctation have been reported in the literature (Table 1 and Supplementary figure S1). It should be noted, however, that there are reports showing no increased risk in developing left ventricular non-compaction cardiomyopathy in the setting of bicuspid aortic valve.Reference Shen, Capoulade and Tastet 20
Table 1. Published cases of left ventricular non-compaction associated with bicuspid aortic valve and aortic coarctation.

In conclusion, the pathogenesis of non-compaction is enigmatic and the clinical implications of the disorder, as well as the optimal management, remain debatable. Concomitant bicuspid aortic valve, aortic coarctation, and non-compaction are a recently defined association that needs further investigation. A major query is whether these entities interact to hasten the potential for adverse clinical events. Repair of the cardiovascular abnormalities seems to restore left ventricular function.
Supplementary Material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1047951119001707.
Acknowledgements
None.
Financial Support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflicts of Interest
None.