Aorta–left ventricular tunnel is a rare congenital anomaly characterised by an extracardiac tunnel that connects the ascending aorta, above the sinotubular junction, to the right or left ventricular cavity. This anomaly is potentially fatal if left untreated, and typically requires surgical correction. Coronary artery anomalies, including atresia of either the right or left coronary artery, have been associated with this defect. We report a rare case of aorta–left ventricular tunnel, ventricular septal defect, and atresia of the right coronary artery with the presence of large right ventricular sinusoids.
Case report
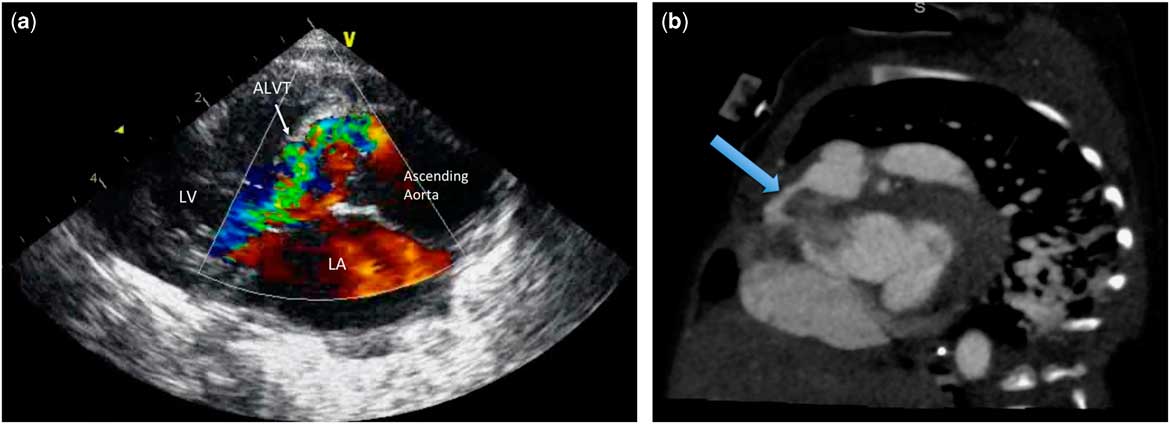
A 35-day-old, 2.3-kg male infant with a known prenatal cardiac anomaly was delivered at 29 weeks of gestation secondary to preterm, premature rupture of membranes. A transthoracic echocardiogram revealed an aorta–left ventricular tunnel with significant left ventricle to aortic flow during systole, flow reversal in diastole, and severe ascending aorta dilation (Fig 1a). There was also a large, muscular ventricular septal defect with low-velocity bidirectional flow across the defect, patent ductus arteriosus, and patent foramen ovale. Biventricular systolic function was normal. The left coronary artery appeared to arise from the left sinus of Valsalva; however, there was concern for origin of the right coronary artery from the pulmonary artery. A CT angiogram of the chest demonstrated right coronary artery atresia with large right ventricular sinusoids that were not filled via the atretic right coronary artery (Fig 1b). The prominent right ventricular sinusoids extended from the rightward margin of the right ventricular outflow tract towards the right atrial groove. There were normal-appearing left main, left anterior descending, and circumflex coronary arteries with no identifiable collateral source from the left coronary system contributing to right ventricular myocardial perfusion. Clinically, the patient had severe aortic regurgitation and pulmonary overcirculation. He developed persistent symptomatic heart failure marked by an inability to tolerate feeds and wean from mechanical ventilation, and he required inotropic support. He was therefore referred for surgical intervention.

Figure 1 ( a ) Transthoracic echocardiogram in the parasternal long-axis view demonstrating a large ALVT with significant aortic to LV flow during diastole and ( b ) CT angiography demonstrating a prominent RV sinusoid extending from the RVOT towards the right AV groove. ALVT=aorta-left ventricular tunnel; AV=atrioventricular; LV=left ventricle; RV=right ventricular; RVOT=right ventricular outflow tract.
Surgical technique
A median sternotomy was performed. There was severe cardiomegaly with dilation of the ascending aorta and pulmonary artery. External examination of the heart revealed a large tunnel that arose from the anterior leftward aspect of the aorta and travelled along the right ventricular infundibulum. An atretic right coronary artery was identified in the atrioventricular groove without evidence of connection to the right coronary sinus. Large right ventricular sinusoids were also visualised (Fig 2a). The patient was systemically heparinised, aortic and bicaval cannulation was performed, and cardiopulmonary bypass was initiated. Upon decompression of the right ventricle, there was no change in heart rate or in the electrocardiogram waveform. The patent ductus arteriosus was ligated, and the patient was cooled to 20°C. Upon spontaneous fibrillation, cardiopulmonary bypass was briefly discontinued, the aortic cross-clamp was applied, and cardioplegia was initially attempted with antegrade root cardioplegia while compressing the left ventricle. However, there was no arrest, and therefore the aorta was transected and direct ostial cardioplegia was delivered via the left coronary artery with prompt diastolic arrest.

Figure 2 ( a ) Intra-operative photograph showing an atretic RCA (*) with large RV sinusoids (arrows), ( b ) a large ALVT (opened by forceps) visualised arising above the right sinus of the aortic valve, and ( c ) ALVT closure using a glutaraldehyde-treated autologous pericardial patch. ALVT=aorta-left ventricular tunnel; RCA=right coronary artery; RV=right ventricular.
No orifice of the atretic right coronary artery could be identified in either the aorta or in the tunnel. The large aorta to left ventricular tunnel was visualised arising above the right sinus of the aortic valve, which had a very hypoplastic right coronary cusp (Fig 2b). A right atriotomy was then performed. The large muscular ventricular septal defect extended from the membranous area to the outlet septum and was repaired with autologous pericardial patch closure. The aortic end of the tunnel was then closed using a glutaraldehyde-treated autologous pericardial patch, with care taken to avoid injuring or distorting the aortic valve (Fig 2c). The patent foramen ovale was then primarily closed. Post-operative echocardiogram demonstrated mild right ventricular and moderate left ventricular dysfunction, no residual ventricular septal defect, mild aortic insufficiency, no aortic stenosis, and no leak from the repaired aorta–left ventricular tunnel. The patient was successfully weaned from cardiopulmonary bypass on epinephrine and milrinone drips for inotropic support and afterload reduction.
Comment
Coronary artery anomalies, including coronary artery atresia and origin of the ostium within the aorta–left ventricular tunnel, have been previously described.Reference Kathare, Subramanyam, Dash, Muthuswamy, Raghu and Koneti 1 – Reference Gundel, Hendrich and Horndasch 4 However, no previous reports have described right ventricular sinusoids in the presence of an aorta–left ventricular tunnel as seen in our patient. The presence of persistent right ventricular sinusoids is thought to develop secondary to suprasystemic right ventricular pressure and has been demonstrated in patients with pulmonary atresia with intact ventricular septum and patients with severe right ventricular hypoplasia.Reference Giglia, Mandell, Connor, Mayer and Lock 5 , Reference Lauer, Fink, Petry, Dunn and Diehl 6
In our patient, there was evidence of an atretic right coronary artery with the presence of large right ventricular sinusoids; however, the patient did not exhibit suprasystemic right ventricular pressures as there was low velocity, bidirectional flow across the ventricular septal defect, and normal oxygen saturations on echocardiogram. Given these findings on echocardiography, there was no physiologic concern for a right-ventricular-dependent coronary circulation. Therefore, we did not believe that coronary perfusion would be compromised with volume unloading and decompression of the right ventricle resulting from closure of both the aorta–left ventricular tunnel and ventricular septal defect.
On the basis of this experience, we believe that a detailed understanding of the coronary anatomy is critical in the perioperative management of aorta–left ventricular tunnel, especially if coronary anomalies are present. Although our patient had evidence of right ventricular sinusoids, there was no physiologic concern for a right-ventricular-dependent coronary circulation. In the instance where right-ventricular-dependent coronary circulation is present, decompression of the right ventricle may significantly affect coronary perfusion, and place the patient at elevated mortality risk after decompression of the right ventricle.Reference Cheung, Richmond, Turner, Bacha and Torres 7 In our patient, preoperative coronary angiography was not performed as the cardiac CT provided adequate detail of the coronary anatomy. However, coronary angiography may be warranted in cases in which the coronary anatomy is not well defined or to determine the presence of right-ventricular-dependent coronary circulation when right ventricular sinusoids are present before right ventricular decompression.
Acknowledgements
None.
Financial Support
This research received no specific grant from any funding agency or from commercial or not-for-profit sectors.
Conflicts of Interest
None.
Ethical Standards
This manuscript does not involve human and/or animal experimentation.