


Coarctation of the aorta accounts for 5–8% of all congenital heart defects. In the neonatal period, surgery is the treatment of choice for primary coarctation. However, surgical treatment in very or extremely low birth weight neonates is challenging and carries a high risk of complications. The authors describe successful interventional treatment of coarctation of the aorta in a preterm neonate weighing 670 grams.
Case report
A male neonate from the first pregnancy was born as the first twin through caesarean section because of threatening asphyxia in the 28th week of gestation. The patient's weight was 580 grams and he received 5 points in the Apgar scale. Prenatally, twin-to-twin transfusion syndrome had been diagnosed, with the described neonate being the donor. Successful laser therapy had been performed. Owing to prematurity, hypotrophy, heart and respiratory failure, the patient required immediate intubation and catecholamine administration. Echocardiography showed patent ductus arteriosus with a large left-to-right shunt, which did not close despite pharmacological treatment. On the 12th day of life, the patient underwent surgical ligation of the patent ductus arteriosus with subsequent clinical stabilisation and withdrawal of catecholamines. After 6 days, the patient's general condition deteriorated, with signs of heart failure and anuria. Echocardiography revealed critical coarctation of the aorta with a diameter of 2 millimetres and peak gradient in Doppler study of 48 millimetres of mercury. Additional symptoms of necrotising enterocolitis and coagulation disorders complicated the clinical course. Owing to continuous worsening of general status with escalated heart failure symptoms, the patient was prepared for percutaneous balloon angioplasty.
To ensure appropriate temperature during the intervention, the patient was placed in an open incubator with overhead and mattress heating and continuous temperature monitoring. These precautions allowed only for right lateral angiograms. The intervention was performed under general anaesthesia with surgical cutdown of the right common carotid artery. Aortography and continuous pullback arterial pressure measurement were done. Critical coarctation to 1.5 millimetres was confirmed with post-stenotic dilatation to 4.9 millimetres and systolic pressure gradient between the aortic arch and the descending aorta of 35 millimetres of mercury (Fig 1a). To dilate the site of the stenosis, Tyshak II 5 × 20 millimetre balloon catheter (NuMED, Hopkinton, New York, United States of America) was chosen; however, under the pressure of 5 atmospheres the balloon did not expand fully (Fig 2a). The second attempt with high-pressure Falcon Forte 4.5 × 14 millimetre catheter (Invatec S.p.A., Roncadelle, Bs, Italy) and 12 atmospheres of pressure was successful. The site of the stenosis was dilated to 3.6 millimetres and the systolic pressure gradient decreased to 8 millimetres of mercury. Control echocardiography showed no coarctation and normal flow in the abdominal aorta.

Figure 1 Aortography in the right lateral projection presenting coarctation of the aorta: (a) before the intervention and (b) after balloon angioplasty.
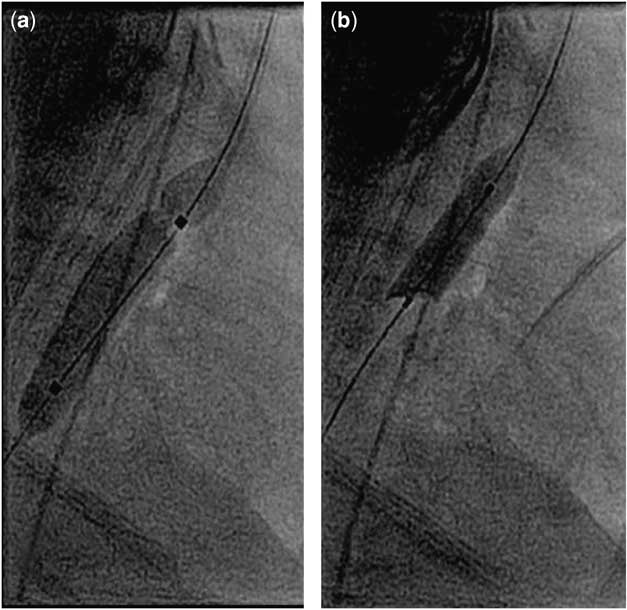
Figure 2 Balloon angioplasty of the aortic coarctation. Inflated balloon catheters: (a) Tyshak II 5 × 20 millimetres and (b) Falcon Forte 4.5 × 14 millimetres.
In the first few hours after the intervention, the patient remained in critical condition with disturbances of peripheral blood flow in lower extremities and anuria. For 4 days, he required catecholamines and diuretics to force the diuresis. In the following days, the patient improved progressively and gained weight. In control echocardiography, no signs of recoarctation were noted.
In 145 days of follow-up, the patient remains stable with no symptoms of heart failure and no recurrence of the stenosis with an actual body weight of 2700 grams.
Discussion
In coarctation, the anatomical isthmus, distal to the origin of the left subclavian artery, is stenosed. It can occur as an isolated disease or in constellation with other cardiovascular defects. In the neonatal period, it very often coexists with a patent ductus arteriosus and hypoplasia of the aortic arch. Patent ductus arteriosus secures right-to-left blood flow from the main pulmonary artery to the aorta below the stenosis. The lack of such communication leads to rapid escalation of heart failure symptoms, oliguria up to anuria, metabolic acidosis, and finally to cardiogenic shock. Therefore, it requires immediate surgical or interventional treatment.Reference Cabrera, Gutiérrez, Pastor, Alcíbar and Martínez 1
Surgery remains the standard treatment in case of native coarctation in neonates. The preferred technique of operation is to excise the site of the stenosis and to create extended end-to-end anastomosis. This strategy allows for the reduction of recoarctation. Low weight is not a contraindication to surgery; however, it augments significantly the risk of complications.Reference Sudarshan, Cochrane, Jun, Soto and Brizard 2 , Reference Alkan-Bozkaya, Türkoğlu and Akçevin 3 The most frequent complication after surgical treatment of coarctation is recoarctation, which occurs in up to 40% of patients.Reference Burch, Cowley and Holubkov 4
Percutaneous balloon angioplasty may be considered an alternative treatment in selected, even low birth weight, neonates with coarctation.Reference Rothman, Galindo, Evans, Collazos and Restrepo 5 , Reference Schamberger and Lababidi 6 During expansion of the balloon catheter, the intimal and medial layers of the stenosed aorta are disrupted with resultant healing. It enables successful and long-lasting dilatation of the vessel. To achieve this, low- and/or high-pressure balloon catheters are used with a diameter exceeding not more than 2 millimetres the diameter of the aorta above the site of the stenosis or equal to the diameter of the descending aorta on the level of the diaphragm. Bigger balloon catheters may produce disruption of the whole wall of the aorta and finally may lead to formation of an aneurysm. The risk of such complications ranges from 0% to 17%, and in most cases aneurysms are small and do not require treatment, but close follow-up. The rate of complications after balloon angioplasty in patients with native and recurrent, post-operative coarctation is similar. Adhesions after previous surgery may mitigate against rupture of the aorta; however, in this patient the short interval between ductal ligation and balloon angioplasty makes it less probable. Successful percutaneous treatment of low birth weight patients has been reported with short- to mid-term follow-up free from restenosis; however, in patients under 6 months of age the risk of recoarctation is up to 50%.Reference Rao, Jureidini, Balfour, Singh and Chen 7 , Reference Liang, Su and Chung 8
In patients with low weight, it is very important to obtain secure vessel access without the risk of complications. Surgical cutdown of the carotid artery reduces the risk of artery damage and thromboembolic sequel in comparison with cannulation of the femoral artery.Reference Sutton, Lock and Geggel 9 Moreover, in these patients it is important to ensure stable temperature comfort during the whole procedure of obtaining surgical vessel access, performing balloon angioplasty, and closure of the wound. In patients with body weight less 1500 grams, Koch et alReference Koch, Buheitel, Gerling, Klinge, Singer and Hofbeck 10 obtained vascular access on a neonatal open care system and then transferred patients to a catheterisation laboratory. In this case, the authors used an open incubator to maintain adequate body temperature and to minimise the risk of hypothermia. However, this brought the inconvenience of performing diagnostic angiograms and the intervention in only one lateral projection without the opportunity to change projections.
Conclusions
The reported successful balloon angioplasty of native coarctation of the aorta in a preterm neonate with extremely low weight of 670 grams and multiple organ failure is an example of interventional treatment as an alternative to surgery.
Supplementary material
The supplementary material referred to this article is available online at http://www.journals.cambridge.org/CTY.



