


Although coarctation of the aorta usually presents in infancy, untreated patients may have complications such as hypertension, aortic aneurysm, and cardiac failure in adulthood. Bicuspid aortic valve generally accompanies coarctation of the aorta.Reference Warnes 1 Transthoracic and transoesophageal echocardiography displays an essential role in the diagnosis of both.Reference Houston, Hillis and Lilley 2 , Reference Miller-Hance and Silverman 3 Patients with bicuspid aortic valve and coarctation of the aorta are prone to develop infective endocarditis.Reference Habib, Hoen and Tornos 4
Coarctation of the aorta can be managed either percutaneously or surgically.Reference Egan and Holzer 5 Here we present a case of percutaneously treated coarctation of the aorta complicated with infective endocarditis of the aortic valve, thoracic aortitis, and thoracic mycotic aneurysm.
Case presentation
A 26-year-old man was referred to our clinic for suspected infective endocarditis. He had been complaining of fever and chills for 7 days. He had a medical history of hypertension, bicuspid aortic valve, and aortic coarctation for which he underwent an unsuccessful attempt at aortic balloon angioplasty a month ago. On physical examination, he had 38.6°C fever, slight tachycardia (105 beats per minute), 160/70 millimetres of mercury blood pressure in the upper extremity and 100/55 millimetres of mercury in the lower extremity, and a 2/6 diastolic murmur most evident over the aortic point. The electrocardiography showed sinus tachycardia with left axis deviation. Telecardiography was normal. Laboratory data showed increased leukocyte count (22,000 per cubic millimetre), C-reactive protein (87 milligrams per decilitre), erythrocyte sedimentation rate (110 millimetres), glutamate oxalacetate transaminase (96 units per litre), alanin amino transferase (120 units per litre), and urea (66 milligrams per decalitre). Other laboratory parameters were within normal limits. Transthoracic echocardiography revealed mildly calcified bicuspid aortic valve, moderate aortic regurgitation, and an isthmus stricture of the descending aorta (Fig 1a). The transoesophageal echocardiography examination showed vibrating echodense vegetation located on the bicuspid aortic valve (Fig 1b). Furthermore, echodense vibrating vegetations were also evident in post-stenotic area distal to the coarctated segment with mycotic aneurysm (Fig 2, Supplementary Movie 1). Therapeutic antibiotherapy with ceftriaxone and gentamycin regimen was started on the patient until the results of blood cultures were obtained. Urine and upper and lower respiratory tract cultures were negative, but methicillin-resistant staphylococcus aureus was revealed in six successive blood cultures. Antibiotherapy was changed to vancomycin and gentamycin regimen, and within 5 days under this antibiotherapy regimen symptoms started to resolve, and leukocyte and C-reactive protein values started to decline. The patient underwent unsuccessful operation on the 34th day of admission and died during operation.
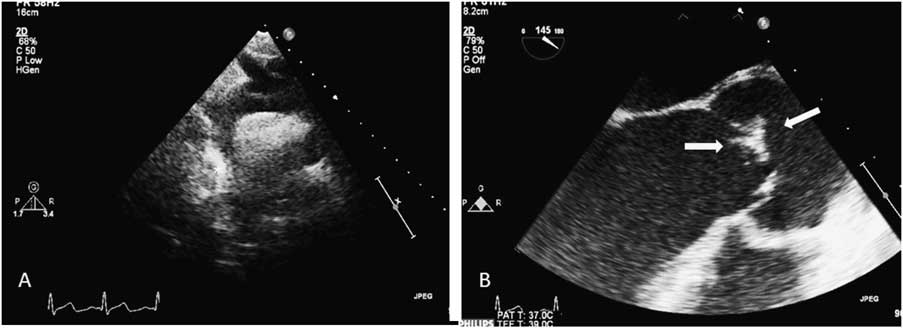
Figure 1 (a) Asterisk indicates an isthmus stricture of the descending aorta. (b) The transoesophageal echocardiography examination showed vibrating echodense vegetation (arrows) located on the bicuspid aortic valve.
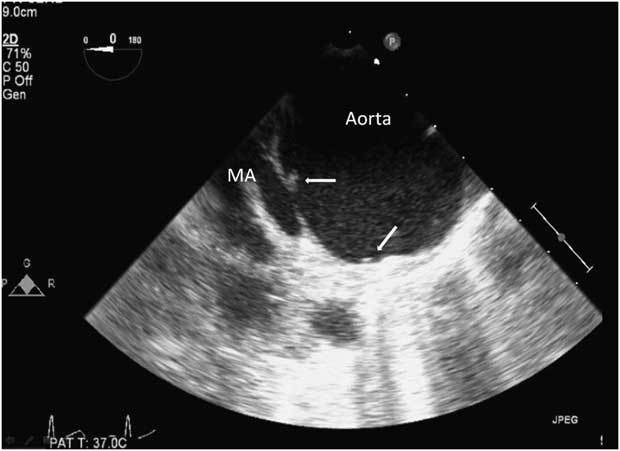
Figure 2 Echodense vibrating vegetations (arrows) were also evident in the post-stenotic area distal to the coarctated segment with mycotic aneurysm (MA) on transoesophageal echocardiographic examination.
Discussion
Coarctation of the aorta is a rare congenital anomaly. Infective endocarditis affecting the coarctation of the aorta also affects the aortic valve.Reference Sanyal, Jadish and Thapar 6 , Reference Garcia, Maroto and Rivera 7 Infective endocarditis alone bears high mortality and morbidity rates.Reference Habib, Hoen and Tornos 4 Moreover, complicating arteritis or endarteritis increases the mortality rate further.Reference Habib, Hoen and Tornos 4 , Reference Sanyal, Jadish and Thapar 6 , Reference Garcia, Maroto and Rivera 7 Vegetations usually presented at the low-pressure site.Reference Habib, Hoen and Tornos 4 Thus, vegetations in coarctation of the aorta are usually located after the coarctated segment.Reference Habib, Hoen and Tornos 4 Mycotic aneurysm of the aorta is an unusual complication of aortitis requiring early intervention.Reference Pasic 8 However, there are controversies about the length of antimicrobial therapy and the surgical technique.Reference Sanyal, Jadish and Thapar 6 – Reference Pasic 8 Infective endocarditis usually presents in patients with predisposing conditions. Disruption of the endothelium and colonisation of the disrupted segment are important in the development of infective endocarditis.
Our patient presented with staphylococcus aureus infective endocarditis complicated by thoracic aortitis and mycotic aneurysm formation a month after the unsuccessful percutaneous intervention for coarctation of the aorta. This is the first case reporting so, after percutaneous balloon aortoplasty.
In conclusion, infective endocarditis may cause pericoarctated site complications including aortitis and mycotic aneurysm in patients undergoing percutaneous balloon aortoplasty, as insertion of catheter and balloon may cause traumatic injury at the aortic endothelium predisposing to the implantation of a bacterial colony, resulting in periaortic complications, mortality, and morbidity.
Supplementary materials
For supplementary material referred to in this article, please visit http://dx.doi.org/doi:10.1017/S1047951112000479



