


A 20-year-old woman diagnosed to have a relapse of pulmonary tuberculosis presented with progressively increasing shortness of breath and abdominal distension. The chest X-ray showed extensive fibrocavitary lesions in both lung fields (Fig 1a). Transthoracic echocardiography revealed an enlarged right atrium and ventricle with normal left-sided chambers. There were multiple, well-circumscribed, and calcified nodular lesions along the free wall of the right ventricle, subvalvular apparatus of the tricuspid valve, and right ventricular side of the interventricular septum (Figs 1b and c; Supplementary movie 1). There was an echolucent area in the submitral region of the posterior left ventricular wall suggestive of the presence of an abscess (Fig 1d; Supplementary movie 2). A diagnosis of tubercular granulomatous myocarditis was made. In addition to supportive treatment for heart failure, the patient was started on empirical antituberculosis regimen keeping in view the history of pulmonary tuberculosis. Biopsy was not carried out owing to poor general condition of the patient. Granulomatous myocarditis is rare with tuberculosis and sarcoidosis being common causes. Other causes include syphilis, fungal infection, rheumatoid, Hodgkin's lymphoma and idiopathic. Constant motion of the myocardium is not conducive to the lodgment of tubercle bacilli or to the development of tubercles. The three types of myocardial tuberculosis are nodular, miliary, and diffuse infiltrating form.Reference Robert 1 Myocardial tuberculosis may manifest from congestive heart failure, atrial and ventricular arrhythmias, superior vena caval obstruction, right ventricular outflow obstruction, and sudden cardiac death. High index of clinical suspicion followed by echocardiography and rapid initiation of treatment on lines of multi-drug-resistant tuberculosis and congestive heart failure resulted in good response.
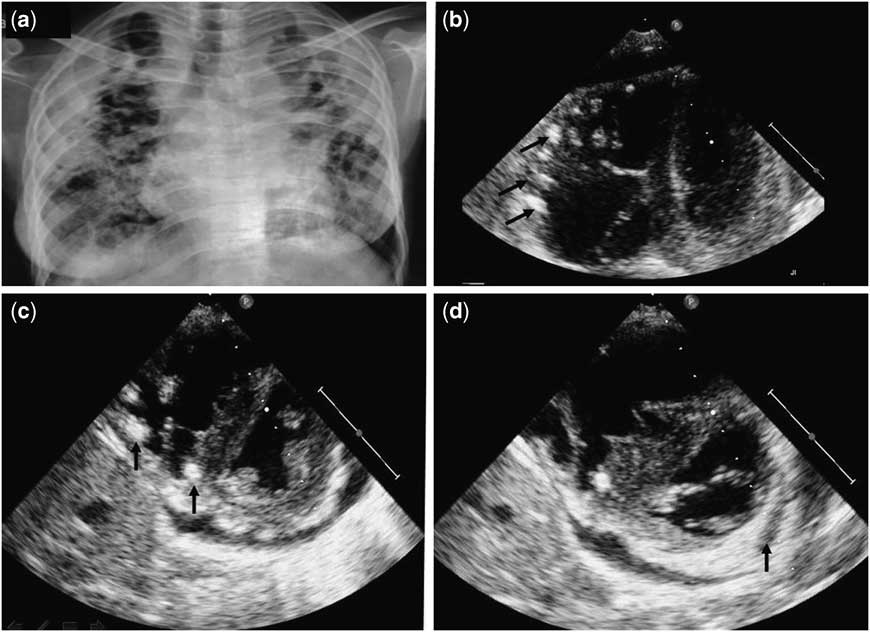
Figure 1 ( a ) Chest X-ray posterior-anterior view showing extensive fibrocavitary lesions in both lung fields with paratracheal and parahilar lymphadenopathy. Note the fibrotic bands producing tenting of the diaphragm. ( b ) Apical four-chamber view – focusing on the right and left ventricles – showing multiple (arrows), well-circumscribed, calcified nodular lesions – tuberculomas – in the free wall of the right ventricle. ( c ) Parasternal short-axis view at the level of the papillary muscle, showing calcified tuberculoma in the interventricular septum (arrows), right ventricle, and mild pericardial effusion. ( d ) Parasternal short-axis view at the level of the mitral valve showing an echolucent space in the submitral region of the left ventricle suggestive of a myocardial abscess (arrow).
Financial Support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of Interest
None.


