Studies have shown an important relationship between the autonomic nervous system, early prognosis of cardiac diseases, and cardiovascular mortality, Reference Lin, Lu and Hsieh1 , Reference Ferreira and Zanesco2 associating a higher propensity for the appearance of lethal cardiac events to an increase in sympathetic autonomic nervous system activity. Reference Peçanha, Paula-Ribeiro, Nasario-Junior and Lima3 The sympathetic and parasympathetic autonomic nervous systems are responsible for the involuntary control of vital physiological functions, such as resting heart rate and stress responses. Therefore, appropriate responses to stress depend on a balance between the sympathetic and parasympathetic systems. Reference Tracy, Ioannou and Baker4 Autonomic dysfunction is mainly characterised by decreased parasympathetic and increased sympathetic activity, Reference Ferreira and Zanesco2 which increases cardiac load and raises ventricular instability, leading to an increased risk of cardiac arrest, infarction, and sudden death. Reference Ferreira and Zanesco2 , Reference Gerritsen, TenVoorde and Dekker5 , Reference Buch, John and Townend6
The evaluation of autonomic dysfunction has recently become widely used through the analysis of heart rate variability (HRV), which provides important information regarding physiological mechanisms, and is considered a reliable, informative, and applicable tool in daily practice for that purpose. Reference Taralov, Terziyski and Kostianev7 HRV represents the variation between consecutive heartbeats and reflects the heart’s ability to adapt to changing circumstances by rapidly detecting and responding to unpredictable stimuli. Lower HRV indicates a lower capacity for autonomic nervous system adjustments Reference Abbate, Arena and Abouzaki8 and has been demonstrated to predict adverse cardiovascular events. Reference da Silva, Massetti and Crocetta9
Some studies have addressed the behaviour of HRV in different conditions such as Duchenne muscular dystrophy, Reference da Silva, Massetti and Crocetta9 Down’s syndrome, Reference de Carvalho, de Abreu and Mustacchi10 , Reference Carvalho, Massetti and Silva11 diabetes, Reference Oliveira, Silva and Christofaro12 and breast cancer, Reference Arab, Vanderlei and da Silva Paiva13 among others. However, the assessment of healthy young people and the effect of physical training on HRV has been little studied. It is known that physical training can improve autonomic dysfunction in pathological conditions. Reference Thayer, Shelby and Jos14 According to a review by Poitras et al, Reference Poitras, Gray and Borghese15 moderate to vigorous physical activity is essential for disease prevention and health promotion; in addition, they state that all activity patterns (sporadic and continuous) can provide benefits. In a recent study, Reference Wu, Kirk, Ohinmaa and Veugelers16 the authors stated that the promotion of programs that encourage physical activity in childhood and adolescence contributes to the prevention of mental disorders, in addition to the prevention of chronic diseases later in life.
The consistent evidence on the cardiovascular, metabolic, and autonomic benefits of acute and chronic physical exercise reinforces physical training as an important non-pharmacological behaviour in the prevention of various pathologies. Reference Parvaneh, Howe and Toosizadeh17 Regular physical activity and a healthy lifestyle have been shown to protect against the occurrence of cardiovascular diseases, reducing not only cardiovascular mortality Reference Byberg, Melhus and Gedeborg18 but also all-cause mortality. Reference Grassi, Mark and Esler19
Previous studies have investigated this issue, but were restricted to traditional aerobic and/or anaerobic exercise routines, or different sports modalities. Reference Figueiredo, Pereira and Neto20 Buchheit et al Reference Buchheit, Simon and Charloux21 and Soares-Miranda et al Reference Soares-Miranda, Sandercock and Vale22 suggested that moderate exercise is sufficient to be associated with higher vagal indexes of the heart and self-estimated health status, with greater cardioprotective effects. Similarly, Bernardi et al Reference Bernardi, Valle, Coco, Calciati and Sleight23 and Melanson Reference Melanson24 concluded that domain measures of resting HRV may distinguish active from inactive individuals; but in both studies, the analysis considered only linear indexes. In this context, Prinsloo et al Reference Prinsloo, Rauch and Derman25 demonstrated that exercise training shows promise as a mechanism to increase HRV; however, further research is required to validate alternative forms of autonomic analysis to investigate changes in HRV after exercise and to evaluate the long-term impact of exercise.
Therefore, the benefits of physical activity are well postulated, but the optimal frequency and intensity levels still remain unclear, especially considering the fractal correlations of HRV. Considering the above, this study proposed to evaluate the linear and non-linear indexes of HRV in healthy young people with different levels of physical activity.
Materials and methods
In this study, we evaluated healthy youngsters from 17 to 30 years of age, with no previous diseases that influenced the protocol, such as physical disabilities, cardiovascular, neurological, and pulmonary diseases, and use of medication. All participants freely consented to the study, which was approved by the Ethics Committee, with number CAAE 0082.0.272.000-09.
Individuals with diabetes mellitus, systemic arterial hypertension, metabolic syndrome, or a parent (father and/or mother) with one of the above, current smokers, and/or drug users with physical dependence were excluded. To characterise the groups, a balance was achieved between men and women. Non-adherence to the protocol, in addition to symptoms such as palpitations and the inability of the individual to remain in resting conditions, without any mental stress for at least 15 minutes, or the use of controlled substance schedules resulted in the exclusion of the individual.
The research was carried out in the Mackenzie Presbyterian University. Individuals were divided according to their degree of physical activity determined by means of the International Physical Activity Questionnaire (IPAQ). Reference Guedes, Lopes and Guedes26 The questions in the questionnaire are related to the activities in the previous week prior to the application of the questionnaire. The participants had their data tabulated and evaluated, and were later classified according to the results of the IPAQ, which divides and conceptualises participants into a number of categories. These include sedentary – does not perform any physical activity for at least 10 continuous minutes during the week; insufficiently active – individuals who practice physical activities for at least 10 continuous minutes per week, but insufficiently to be classified as active; active – complies with the following recommendations: (a) vigorous physical activity ≥3 days per week and ≥20 minutes per session; (b) moderate physical activity or walking ≥5 days per week and ≥30 minutes per session; (c) any added activity: ≥5 days per week and ≥150 minutes per week; and very active – complies with the following recommendations: (a) vigorous physical activity ≥5 days per week and ≥30 minutes per session; (b) vigorous physical activity ≥3 days per week and ≥20 minutes per session and/or walking ≥5 days per week and ≥30 minutes per session. Reference Silva, Bergamaschine, Rosa and Melo27
The questionnaire was given to the subjects, who received verbal guidance to fill it out, as well as a written orientation regarding questionnaire completion, which was attached to the questionnaire. Any doubts were clarified at the time of completion, and the study subjects could not communicate with each other.
Immediately afterward, an HRV evaluation was performed. All heart rate records were performed using a cardiofrequency meter (Polar® RS800CX), previously validated for beat-to-beat heart rate capture and the use of its data for HRV analysis. Reference Gamelin, Berthoin and Bosquet28 , Reference Kingsley, Lewis and Marson29 Before HRV measurements, blood pressure, heart rate, and general condition of the individual were measured. The collection was performed in a controlled environment (room with a stretcher) with a temperature around 22°C, and the individual remained at rest in the lying position. We had special concerns regarding noises that might bother the subjects, who were instructed not to sleep during the evaluation, as well as not talking, not moving in excess, and remaining without any mental stress.
For the analysis of HRV data in dorsal decubitus, 15 minutes were recorded in order to assess at least 1000 consecutive RR intervals (after filtering); only series with >95% of sinus beats were included in the study. Manual filtering was performed in Microsoft Excel to eliminate premature ectopic beats and artefacts; there was no substitution, only the elimination of artefacts. Reference Godoy, Takakura and Correa30 The software used for HRV analysis by linear methods was Kubios HRV, and detrended fluctuation analysis software was used for the non-linear methods. Reference Peng, Havlin, Stanley and Goldberger31
During data analysis, for comparisons between groups (sedentary, insufficiently active, active, and very active), a one-way ANOVA was carried out with the least significant difference post hoc test. The software package used was SPSS, version 20.0 (p<0.05).
Results
Fifty-five subjects were evaluated and classified according to their level of physical activity (IPAQ) in 12 sedentary, 16 insufficiently active, 14 active, and 13 very active subjects. Only one case was excluded because of the inability of the individual to remain in resting conditions and the use of controlled substance schedules.
The groups were similar in terms of blood pressure (systolic and diastolic), heart rate, and respiratory rate at rest, differing only in age from the very active group, which was younger in relation to the others (Table 1). No differences were found between groups for the variables weight and height.
Table 1. General data

S=sedentary; IA=insufficiently active; A=active; VA=very active; N=number of participants; M=male; F=female; SBP=systolic blood pressure; DBP=diastolic blood pressure; HR=heart rate; f=respiratory rate; BMI=body mass index.
* p≤0.05 when comparing Very Active with all other groups, no differences found between the other three groups.
Time domain
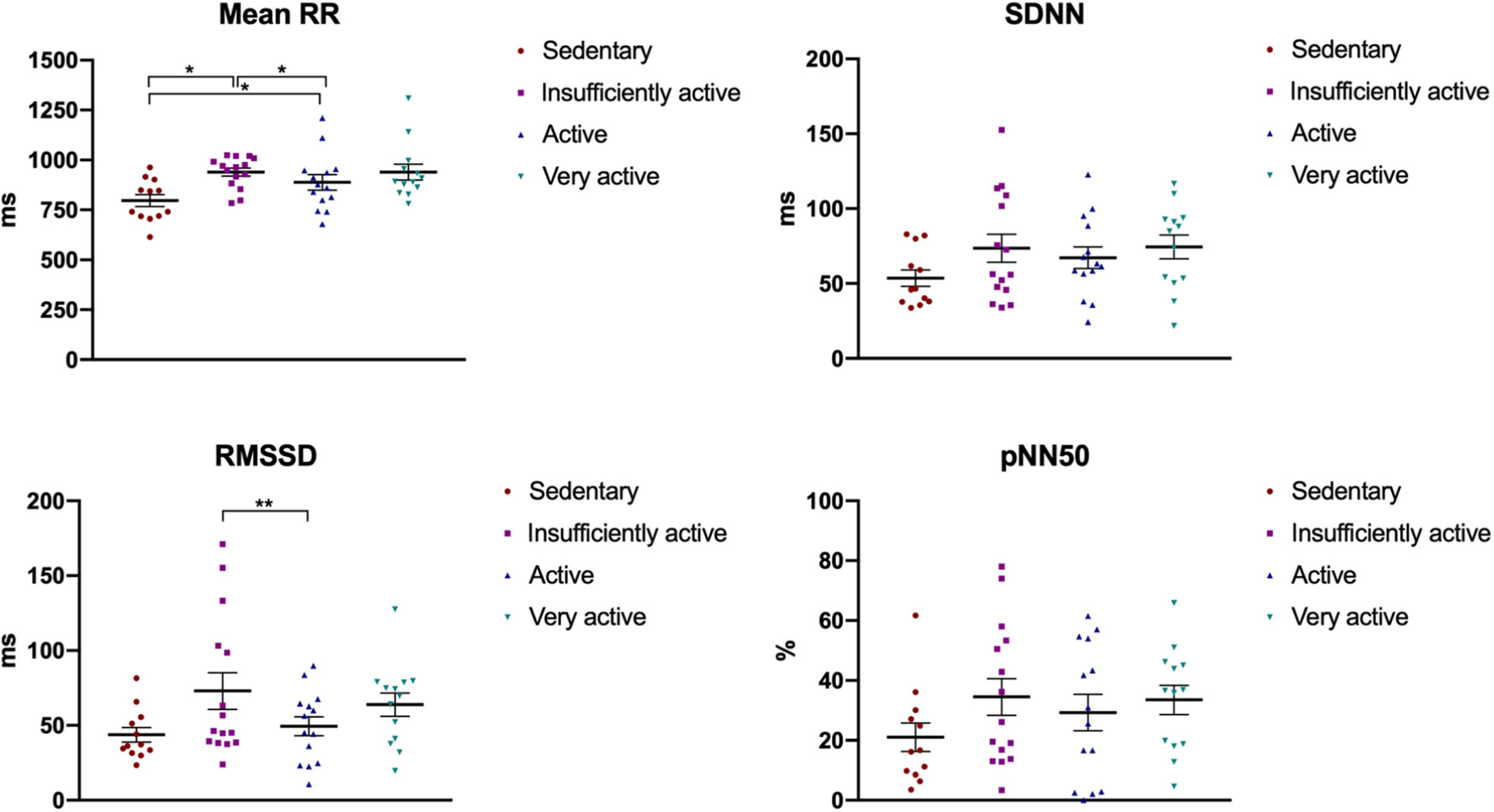
The one-way ANOVA showed statistical significance for mean RR (F3,53=4.0, p=0.013) and marginal significance for rMSSD (F3,53=2.4, p=0.082). No statistical significance was found for SDNN and pNN50. Figure 1 shows the means and standard error bars. The post hoc test showed that, for the sedentary group, the mean RR and rMSSD were significantly lower and the insufficiently active group showed higher means, but significantly only for rMSSD.

Figure 1. Representation of mean and standard error of the variables of the time domain, in the four groups evaluated. *p≤0.05 when comparing sedentary with all other groups, with no differences found between the other three groups. **p≤0.05 when comparing insufficiently active with sedentary and active, with no differences found between the other groups.
Frequency domain
For the frequency domain, the one-way ANOVA showed no statistical significance for any of the variables. The means and standard errors are depicted in Figure 2.

Figure 2. Descriptive values of mean and standard deviation of the variables of the frequency domain, in the four groups evaluated.
Detrended fluctuation analysis
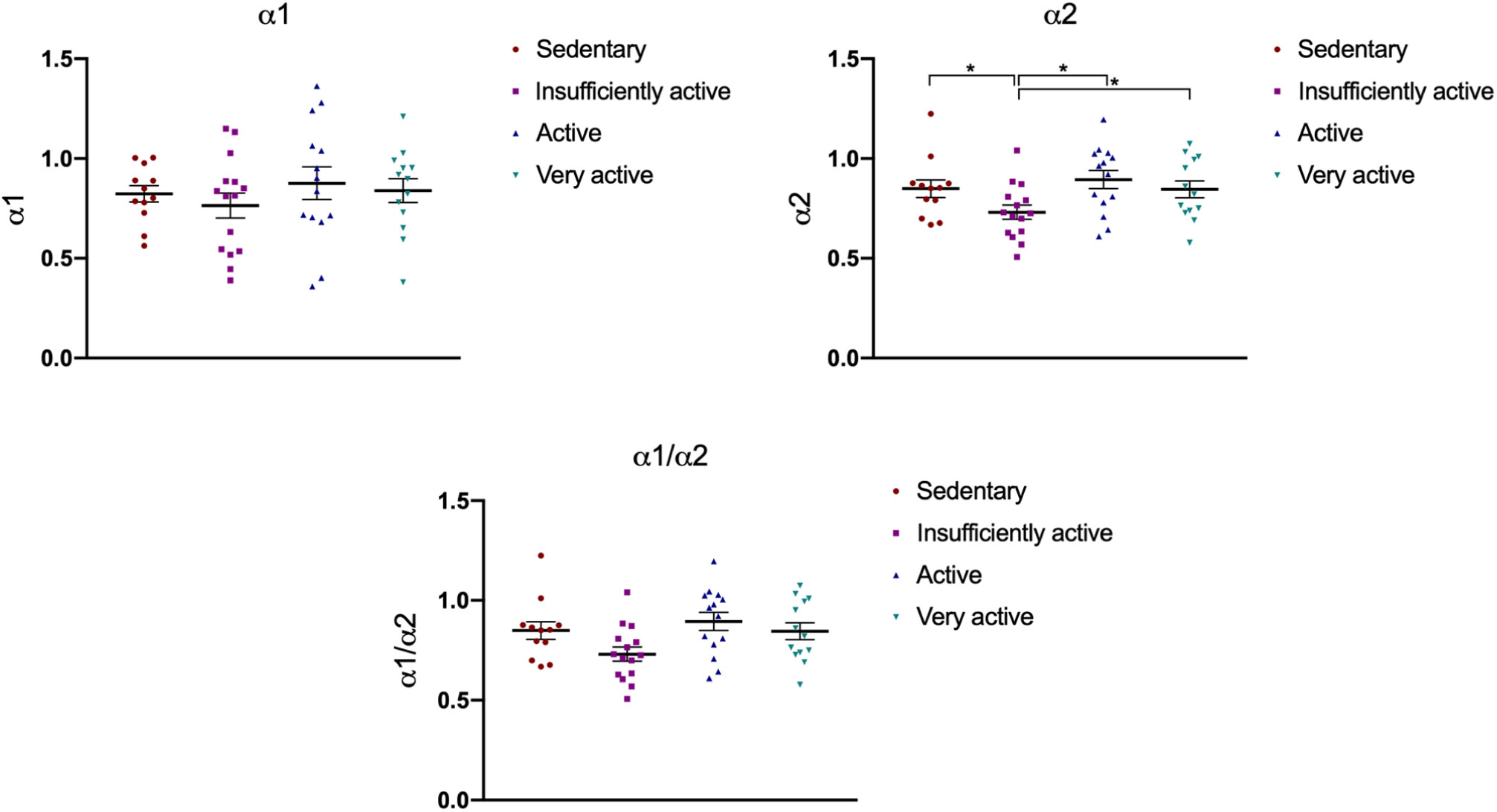
The α1 and α2 exponents of the detrended fluctuation analysis were calculated using the software developed by Peng et al Reference Peng, Havlin, Stanley and Goldberger31 (available at www.physionet.org/physiotools/dfa/#software-for-dfa). Reference Goldberger, Amaral and Glass32 The one-way ANOVA showed statistical significance for α2 (F3,53=2.9, p=0.040). No statistical significance was found for α1 and α1/α1. The post hoc test showed that, for the insufficiently active group, α2 was significantly lower compared with the sedentary, active, and very active groups (Fig 3).

Figure 3. Descriptive values of mean and standard deviation of the variables of the detrended fluctuation analysis, in the four groups evaluated.
*p≤0.05 when comparing Insufficiently Active with all other groups, with no differences found between the other three groups.
Analysis comparing two groups
We combined the “sedentary” and “insufficiently active” subjects into group 1 and the “active” and “very active” subjects into group 2, in order to increase the sample in each group and determine whether the results remained similar. For that, a t-test was performed to compare all HRV indices used in this study and confirmed a significant difference for α2, in which group 1 presented a smaller α2 value (mean±standard deviation, 0.78±0.15) compared with group 2 (0.87±0.16). No significant differences were found for the time or frequency domains.
Discussion
In the present study, we aimed to evaluate the linear and non-linear indexes of HRV in healthy young people with different levels of physical activity. By HRV analysis, it is possible to access relevant information about autonomic nervous system integrity, indirectly and at a low cost. Reference Zuttin, Moreno, César, Martins, Catai and Silva33 – Reference Valenti, Guida and Frizzo35 Although HRV is commonly analysed using linear models, interest in non-linear methods has increased in recent years. This methodology differs from standard approaches because it considers the qualitative properties of a heart rate time series. Reference Perseguini, Takahashi and Rebelatto36 The mechanisms that involve cardiovascular regulation are interconnected in a non-linear theory, and therefore non-linear analysis could provide additional information. Reference Jokinen, Tapanainen, Seppänen and Huikuri37 , Reference Huikuri, Mäkikallio and Perkiömäki38 Non-linear analysis may be more suitable for reflecting changes in the autonomic modulation of biological systems, as there is evidence that the mechanisms involved in cardiovascular regulation probably interact with each other in a non-linear way. Reference Scheff, Griffel, Corbett, Calvano and Androulakis39 It provides additional information on the complexity, or randomness, of a time series, Reference Soares-Miranda, Sandercock and Vale22 and describes elements manifesting behaviours that are extremely sensitive to the initial conditions, or difficult to repeat, but nevertheless are deterministic. Reference Godoy, Takakura and Correa30 One method used for non-linear analysis is detrended fluctuation analysis. This method quantifies the absence or presence of fractal correlation properties in RR intervals. Fractal indices are used to detect slight changes in RR interval dynamics. Furthermore, changes in the fractal correlation properties of long- and short-term dynamics of HRV help clinical professionals to prevent disease development and identify autonomic impairment. Reference de Souza, Cisternas and de Abreu40
Thus, there is a need to use fractal indices for the analyses of different levels of physical activity; physical inactivity is an important risk factor for cardiovascular mortality and morbidity as regular exercise is known to improve health and maintain physical fitness. Reference Panda and Krishna41 In this way, the effects of maintaining physical activity have been related to an increase in the parasympathetic response with a concomitant reduction in sympathetic tone. As an expression of such adaptations, physically inactive individuals often present a lower resting heart rate and greater parasympathetic activity. Reference Migliaro, Contreras and Bech42
The literature points shows that low HRV is associated with a reduced capacity to adjust to environmental demands and increased cardiovascular disease and mortality. Moreover, low HRV is consistently noted in individuals who are sedentary. Reference Buchheit, Simon and Charloux21 , Reference Soares-Miranda, Sandercock and Vale22 , Reference Kawaguchi, Nascimento and Lima43 A generalised increase in sympathetic activity would decrease the duration of RR intervals, reducing HRV. Conversely, the reduction in heart rate by an increase in parasympathetic activity leads to an increase in the duration of RR intervals and an increase in HRV. Reference Vanderlei, Pastre, Hoshi, de Carvalho and de Godoy34
In our study, sedentary individuals presented differences with the other groups only in mean RR, which was lower than in the other groups, reflecting a higher mean heart rate. In turn, the insufficiently active individuals presented differences with the sedentary and active groups regarding rMSSD, as well as α2 in detrended fluctuation analysis for all groups.
Another important finding concerns the values of α2, which were lower in the insufficiently active group, indicating the loss of fractal correlation. However, this technique is not widely applied in clinical practice, a major reason for which might be the lack of practical interpretation, in the face of the large amount of data provided by HRV linear and non-linear analysis. Reference Hoshi, Vanderlei and de Godoy44 We can speculate that our results confirm that the non-linear method better represents the nature of organic systems as described above, considering that the results for the sedentary and insufficiently active subjects (group 1) and active and very active subjects (group 2) confirmed the significant difference in α2, in which group 2 showed values of α2 closer to 1, when compared to group 1, corroborating the loss of fractal correlation in less active subjects.
Detrended fluctuation analysis quantitatively reduces HRV to a simple fractal scaling exponent α. The detrended fluctuation analysis of HRV has been used to evaluate the risk of mortality in various groups. A lower α value is a strong predictor of cardiac and total mortality. Reference Hsin, Yang, Yeih, Shieh and Li45 Therefore, considering the non-linear nature of organic systems, non-linear analysis is necessary, because some information may be lost if only linear methods are applied. These techniques have been shown to be powerful tools for the characterisation of complex systems, like the complexity and fractal scaling properties of the cardiac beat-to-beat series. 46 Silva et al Reference Silva, Pereira and Reis47 and Sen and McGill Reference Sen and McGill48 reported that although α2 is less reported in the literature, it is related to a decrease in the oxygen desaturation index and cardiovascular disease, Reference Silva, Pereira and Reis47 and is strongly related to mortality. Reference Sen and McGill48
Detrended fluctuation analysis calculates the fluctuation of the mean square root of the integral and purifies the time series, allowing the detection of the intrinsic autosomillarity embedded in the non-stationary time series. The detrended fluctuation analysis graph is not strictly linear, but consists of two distinct regions of distinct curves, separated by one point, suggesting that there is a short-term fractal scale exponent (α1) during periods of 4–11 beats (or 4–13), and a long-term exponent (α2) for longer periods (>11 beats). Reference de Carvalho, de Abreu and Mustacchi10 , Reference Acharya, Paul Joseph, Kannathal, Lim and Suri49
An α between 0 and 0.5 indicates that large and small values of the time series are more likely to alternate; α=0.5 corresponds to white noise, in which >0.5 and <1.0 indicates persistent long-range power law correlations such that a large (compared with the average) interbeat interval is more likely to be followed by large interval and vice versa. α=1 represents 1/f noise; for α≥1, correlations exist but cease to be of a power law form and α=1.5 indicates Brownian noise or random walk. Reference Peng, Havlin, Stanley and Goldberger31 , Reference Acharya, Paul Joseph, Kannathal, Lim and Suri49 , Reference Hoshi, Pastre, Vanderlei and Godoy50 In summary, for healthy individuals, the α1 value tends to 1 (unity) and is higher than the α2 value. Reference Vanderlei, Pastre, Júnior and de Godoy51
Regarding the square root of the mean of squared differences between successive beat intervals (rMSSD), it positively correlates with relative parasympathetic dominance over cardiac rhythm. Reference da Silva, Massetti and Crocetta9 In this sense, the individuals of the insufficiently active group presented parasympathetic dominance, which did not differ from the very active group. This result is similar to the findings of Rossi et al Reference Rossi, Vanderlei and Bernardo52 that assessed linear and detrended fluctuation analysis indices of HRV of people with chronic obstructive pulmonary disease and showed increases in rMSSD and decrease in α2 (indeed, more accentuated in the control group). The authors stated that this result is strongly associated with alterations in the respiratory rate, and we can only speculate that our results are due to respiratory patterns that were not assessed in the subjects of this study, since it occurred only in the insufficiently active group and not in the sedentary or very active groups.
Conversely, Soares-Miranda et al Reference Soares-Miranda, Sandercock and Vale22 described studies that have found no positive association between physical activity and HRV, assessed indirectly via questionnaires. This type of evaluation has an inherent bias. Despite advances in physical activity assessment methods, it is still a great challenge to evaluate physical activity, especially in low- and middle-income countries. Direct methods of measuring physical activity have been used, but costs are still high, making this unfeasible for use in countries such as Brazil. Despite the problems related mainly to subjective assessment and estimation errors, questionnaires remain the most used option for studies. Reference Garcia, Osti, Ribeiro and Florindo53 In Brazil, the main questionnaire is the IPAQ, which is a questionnaire that assesses physical activity in a typical week or in the last 7 days by investigating minutes of physical activity (moderate, vigorous, and walking). However, it was demonstrated that this instrument overestimated physical activity compared with objective measurements and that the instrument was a relative indicator of physical activity. Reference Garcia, Osti, Ribeiro and Florindo53 , Reference Zanchetta, Barros and César54 In this way, it is essential to use a valid instrument that is easy to apply and inexpensive, allowing for the comparison between surveys conducted in different locations. The IPAQ was proposed by the World Health Organisation, aiming to provide a tool to measure the level of physical activity that could be applied in different regions and cultures, Reference Zanchetta, Barros and César54 and it was validated in Brazil. Reference Guedes, Lopes and Guedes26 Therefore, we hypothesised that the limitations of the questionnaire may have caused the change in rMSSD for the under-active groups since the classification should not have been adequate for this population.
According to Haskell et al, Reference Haskell, Lee and Pate55 it is recommended to perform ≥30 minutes of moderate-intensity aerobic physical activity 5 days per week, or 20 minutes of vigorous-intensity aerobic physical activity 3 days per week to promote health. According to the IPAQ, an insufficiently active individual does not comply with these recommendations, so we can assume that the responses were over- or underestimated by the research participants.
Cross-sectional studies show that greater overall levels of physical activity and aerobic fitness are associated with higher values of traditional indices of HRV. What is not clear from these studies is how different elements of physical activity (such as intensity) are associated with HRV. This trend was also shown by Lopes et al Reference Lopes, Pereira, Reboredo and Castro56 who observed in young individuals that HRV was not significantly modified by the type of physical training studied. However, with training, there was an increase in all variables used for HRV analysis, indicating a change in autonomic modulation, although these changes were not statistically significant. In a study by Dutra et al, Reference Dutra, Pereira, Tezini, Mazon, Martins-Pinge and Souza57 they investigated whether aerobic capacity interferes with the autonomic modulation of HRV and whether gender differences exist. The results suggest that aerobic physical capacity does not interfere with HRV modulation; however, the cardiac modulatory balance differs between genders and is characterised by a greater influence of the autonomic vagal component in women and by the sympathetic component in men.
In a study by Peçanha et al, Reference Peçanha, Paula-Ribeiro, Nasario-Junior and Lima3 although they compared levels of physical activity among healthy individuals, the authors focused their analyses on the post-training period and also confirmed the increase in HRV in trained individuals. The authors described the need for more studies to confirm the potential cardioprotective effect of physical training on the cardiovascular system in clinical populations through a longitudinal design.
Sotiriou et al Reference Sotiriou, Kouidi, Samaras and Deligiannis58 and Kawaguchi et al Reference Kawaguchi, Nascimento and Lima43 observed that the HRV of athletes is higher than that in sedentary individuals, indicating that physical activity may be able to increase the physiological capacity of the cardiovascular system to vary heart rate and, consequently, better adapt to changes or stimuli of the external environment. The HRV can be useful for the assessment of cardiac autonomic modulation in sports cardiology. Furthermore, our data, together with the evidence shown by the other studies cited in this discussion, provide a supporting rationale for a polarised model of training, showing that training phases with increased time spent at high intensity suppress parasympathetic activity, while low-intensity training preserves and increases it. As such, periodised low-intensity training may be beneficial for optimal training programming. Reference Plews, Laursen, Kilding and Buchheit59
As limitations of the study, we can cite the lack of assessment of metabolic variables, such as respiratory rate and oxygen saturation; we believe that future studies should assess these variables. As a second limitation, we did not use another measurement of the level of physical activity to improve the distribution of the groups.
We conclude that young, healthy, sedentary individuals present an increased heart rate and that insufficiently active subjects present a decrease in the fractal correlation and increased parasympathetic activity.
Acknowledgements
We would like to thank Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil.
Financial support
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil: Finance Code 001.
Conflicts of interest
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation (Resolution CNS 466/12) and with the Helsinki Declaration of 1975, as revised in 2008, and have been approved by the institutional ethics committee (Mackenzie Presbyterian University, with number CAAE 0082.0.272.000-09).