The long-term survival and functional state after Classical Fontan operation is limited by late complications including Fontan pathway obstruction, right atrial dilatation, atrial arrhythmias, poor exercise capacity, failing ventricular function, and protein-losing enteropathy.Reference Cromme-Dijkhuis, Hess and Hahlen1
A study by Mavroudis and Deal and their associatesReference Mavroudis, Deal and Backer2 suggests that conversion to Total Cavo Pulmonary Connection with concomitant arrhythmia surgery and use of an atrial antitachycardia pacemaker might be the most promising solution. Despite the early to mid-term results being encouraging, there is no clear indication for the timing of surgery. We present our experience with Fontan conversion and concomitant arrhythmia surgery from a single centre, which emphasises the need for optimal timing of this surgery.
Patients and methods
There were 15 patients who underwent conversion to Total Cavo Pulmonary Connection with arrhythmia surgery for late complications after the classical Fontan procedure between the years 2002 and 2009. The perioperative patient characteristics are summarised in Table 1.
Table 1 Perioperative details.

Refractory atrial arrhythmia despite optimal medical management was the main indication for Fontan conversion in this group of patients. Atrial arrhythmias were considered refractory when there were symptomatic arrhythmia recurrences despite treatment with maximum therapeutic doses of beta-blockers, calcium channel blockers, flecainide, and amiodarone. A minimum of two anti-arrhythmic drugs were given at a time for a duration of at least 24 months to optimise medical management.
There were 14 patients (93%) with atrial arrhythmias refractory to medical management. The average duration of medical therapy in these patients was 80.6 plus or minus 57.5 months. The indication for Fontan conversion in one of the fifteen patients is effort intolerance and progressive right atrial enlargement with a massive right atrial thrombus. She did not have refractory arrhythmia, but Holter monitoring suggested frequent atrial ectopics and runs of atrial tachycardia.
All 15 patients had effort intolerance and a markedly dilated right atrium with venous stasis and spontaneous contrast on echocardiography. There were two patients with a Thrombus in the right atrium. There were 10 patients who were on oral anticoagulant therapy. Cardiac catheterisation demonstrated anastomotic site obstruction in four out of the 15 patients. Catheterisation could not be performed in two patients with a right atrial thrombus. An electrophysiological study was performed in seven patients, but none of them were subjected to radiofrequency ablation in view of the massive right atrial enlargement requiring surgical right atrial reduction.
Surgical technique and perioperative management
Right atrial reduction was performed in patients with a pre-operative echocardiographically measured right atrial short-axis dimension exceeding normal values by at least 50% – atrial dimensions indexed to body surface area. Monopolar irrigated radiofrequency ablation (Cardioblate Surgical Ablation System, Medtronic Inc., Minneapolis, United States of America) was performed in all patients. We used an irrigation flow rate of 5 millilitres per minute, power of 30–40 watts (40 watts for the thicker atrial wall), pen movement of 0.5 centimetres per second, and ablation time of 10 seconds for each cycle. Ablation lines and surgical incisions, which were previously reported, were performed in a standard way in the right and left atria.Reference Giamberti, Chessa and Abella3, Reference Giamberti, Chessa and Foresti4 In patients with severe atriomegaly, the right atrial appendage was excised and a large part of the free wall was removed. A biatrial approach, similar to the Cox–Maze III procedure, was performed in six patients, and the right-sided Maze procedure (ablation lines in the right atrium only) in nine patients. At the end of the operation, epicardial wires were placed on the right atrium and left ventricle (main systemic ventricle) in all patients. Intraoperative pacemaker implantation was performed when indicated by severe bradycardia in seven patients (47%), which included replacement of previously implanted pacemakers in two patients. Aortic cross-clamp time was extended by 15 minutes in cases where a left atrial ablation was performed. The excision and ablative incision in the right atrium were performed with the aorta unclamped. An extra cardiac type of Total Cavo Pulmonary Connection was performed in 14 patients, whereas one patient with Dextrocardia had Lateral tunnel Fontan conversion. Prophylactic amiodarone (5 milligrams per kilogram per day) was administered during the immediate and early post-operative period. Electrophysiological studies or cardiac catheterisations were not performed before discharge in any of these patients.
During follow-up, patients were assessed by clinical examination, echocardiography, 12-lead electrocardiography, and Holter monitoring. Patients with permanent pacemakers had them interrogated at regular intervals for atrial tachycardia events.
Statistical methods
Categorical data were analysed using χ 2 test and Fisher's exact test.
Results
Early mortality
There were two in-hospital deaths (13.3%) with only one probably related to persistent post-operative arrhythmia. This was a 21-year-old male who had refractory atrial fibrillation, a worsening of the atrioventricular valve regurgitation and ventricular function, and who died on the tenth post-operative day with low cardiac output and multi-organ dysfunction. He had permanent atrial fibrillation of 13 years’ duration. The second death involved a 35-year-old male patient who had uncontrollable haematemesis from pre-existing oesophageal varices. He died on the 23rd post-operative day and remained in sinus rhythm until death. Unfortunately, he was anticoagulated as per our post-operative protocol.
Post-operative arrhythmias
Haemodynamically significant early post-operative arrhythmias occurred in seven patients (46.6%) with none of them being new onset arrhythmia. Except one patient who died, all the other six patients responded to treatment with either anti-arrhythmic drugs or cardioversion.
At the time of discharge, all the 13 surviving patients were haemodynamically stable. There were five patients who were in sinus rhythm. Anti-arrhythmic drugs were continued for 3 months for all patients, including those in sinus rhythm at the time of discharge.
Late recurrence of arrhythmia with a need for prolonged anti-arrhythmic drug therapy was present in two patients among the 13 survivors (15.30%). There was one patient who underwent radiofrequency ablation – retrograde approach through the aorta – after 18 months of drug therapy, was successfully ablated, and whose medications were stopped. The second patient had recurrence of arrhythmia from six months after surgery. He continues to be on anti-arrhythmic agents and his arrhythmia is well under control with drug therapy.
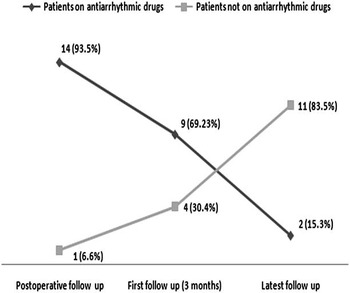
The number of patients requiring anti-arrhythmic agents pre-operatively, at 3 months, and at mid-term follow-up for the complete series is shown in Figure 1. There was a reduction in the number of patients requiring anti-arrhythmics at first follow-up compared with the pre-operative period (p = 0.08, Fisher's exact test). Patients continued on anti-arrhythmic drugs were significantly less (p<0.05) at the mid-term follow-up compared with the pre-operative period. None of the seven patients who had pacemaker implantation had any pacemaker-related problems during follow-up.

Figure 1 Change in need for anti-arrhythmic medications during follow-up (n = 15)
Late death/need for cardiac transplantation/organ dysfunction
The mean follow-up period was 56 plus or minus 19 months. There was no late death or cardiac transplantation. Of the two patients who had late recurrence of arrhythmia, one has progressive worsening of the ventricular function, exercise limitation, and cardiac cirrhosis on follow-up, although the arrhythmia is under control with drugs.
Discussion
Classical Fontan connection and its modifications always included the right atrium as a functional part of the Fontan pathway. Right atrial dilatation and hypertension occurs with time leading to the pathological Fontan state. Conversion to total cavopulmonary anastomosis began after initial reports by de Leval in 1988.Reference de Leval, Kilner, Gewilling and Bull5 With conversion to the lateral tunnel type of Total Cavo Pulmonary Connection, late recurrence of arrhythmias was reported to be 76%Reference de Leval, Kilner, Gewilling and Bull5, especially when there was no arrhythmia treatment protocol or concomitant arrhythmia surgery.
Conversion to the extracardiac type of Fontan with concomitant arrhythmia surgery has led to the effective control of arrhythmias in the long term. Mavroudis et alReference Mavroudis, Deal and Backer2 reported an incidence of late death/need for transplantation of 5.4% and late recurrence of arrhythmia of 15.7% with this strategy.
Our current indications for Fontan conversion are mechanical pathway obstruction or atrial dilatation with symptomatic arrhythmias uncontrolled with multiple drug therapy or controlled at the expense of drug side effects. There was no late death or need for cardiac transplantation in our series. The late recurrence of arrhythmia is 15.30%, similar to the report by Mavroudis et alReference Mavroudis, Deal and Backer2 The arrhythmias that have recurred late after Conversion operation are well controlled with medications compared to their refractory pre-operative status. There is a significant reduction in the need for anti- arrhythmic agents from 92.4% to 15.2% in the mid-term follow-up, similar to the results reported by Sheikh et al.Reference Sheikh, Tang and Roman6
Among the various late complications of Classical Fontan operation, atrial arrhythmias contribute significantly to mortality in the long term.Reference Ghai, Harris, Harrison, Webb and Siu7 The addition of arrhythmia surgery to the Fontan conversion procedure has definitely led to the effective control of refractory arrhythmias and improved survival in these patients.Reference Mavroudis, Deal and Backer2 However, achieving a stable sinus rhythm in the early post-operative period as well as controlling late recurrence of arrhythmia still remains a challenge after Fontan conversion.
In our series, we found difficulty in achieving stable sinus rhythm post-operatively in patients who had prolonged duration of pre-operative arrhythmia. During the early post-operative period, only one out of 15 patients had stable sinus rhythm. Patients who had difficulty in achieving sinus rhythm post-operatively were found to have prolonged pre-operative arrhythmia of more than 10 years, whereas the average duration of pre-operative arrhythmia among patients who had stable sinus rhythm on mid-term follow-up was 53 (20–86) months.
There was one patient who died in the early post-operative period and two patients with late recurrence of arrhythmia who had prolonged duration of pre-operative arrhythmia of more than 10 years. Our observation in this group suggests that delay in Fontan conversion in the presence of arrhythmias increases mortality and morbidity during the perioperative period. However, to compare and prove this fact, we do not have a control group with an equal number of classical Fontan patients who are only medically managed. Our finding is similar to the report by Kawahira et alReference Kawahira, Uemura, Yagihara, Yoshikawa and Kitamura8 who reported similar difficulty after Fontan conversion and arrhythmia surgery.
In our experience, the duration of pre-operative arrhythmia seems to have an adverse impact on the post-operative outcome as noted in previous reports.Reference Kawahira, Uemura, Yagihara, Yoshikawa and Kitamura8, Reference Koh, Yagihara and Uemura9 This emphasises the need to optimise the timing of Fontan conversion to improve the long-term results in terms of arrhythmia control. At present, there are no reliable predictive indications or criteria available for timing Fontan conversion in relatively asymptomatic or less symptomatic patients. There is a complete lack of data on conversion in asymptomatic patients with arrhythmias, well controlled with medications. Our series also did not have any asymptomatic patient.
Prophylactic conversion regardless of symptoms, arrhythmias, or abnormal haemodynamics is under consideration in the present era, but is yet to be studied in a large cohort of patients. In recent reports,Reference Koh, Yagihara and Uemura9, Reference Wong, Davlouros, Li, Millington-Sanders, Francis and Gatzoulis10 two simple electrocardiographic markers, namely the P wave duration and dispersion, were found to be informative when considering conversion procedure before the onset of sustained tachyarrhythmia.
Reasonable functional status or temporary control of arrhythmia with medications should not be reasons for postponing conversion procedure. Identifying the early markers of sustained atrial arrhythmias and converting the classical Fontan connection before the onset of sustained atrial arrhythmia appear to be the strategies most likely to improve the results of Fontan conversion and concomitant arrhythmia surgery. Simple clinical markers like exercise capacity, electrophysiological markers like P wave characteristics, morphological markers like right atrial size, and biochemical markers like Brain natriuretic peptide can guide us in deciding the timing of Fontan conversion. More investigational work needs to be done to assess the reliability of these markers and to develop clinical criteria for optimal timing of Fontan conversion.