


Non-invasive assessment of right ventricular function is difficult due to its complex geometry.Reference Geva, Powell, Crawford, Chung and Colan 1 Right ventricular function is especially difficult to evaluate in patients with repaired tetralogy of Fallot due to aneurysmal right ventricular outflow tract dilatation. These aneurysms are non-contractile and have paradoxical motion, increasing right ventricular volume while simultaneously decreasing the right ventricular ejection fraction. In order to account for this, Kutty et al used cardiac MRI to segment the right ventricle in patients with repaired tetralogy of Fallot and analysed the right ventricular sinus and infundibulum separately.Reference Geva, Powell, Crawford, Chung and Colan 1 , Reference Kutty, Zhou, Gauvreau, Trincado, Powell and Geva 2 This allowed for the assessment of right ventricular sinus ejection fraction, which is presumably a measure of the “true” right ventricular myocardial function in repaired tetralogy of Fallot patients; however, this method of segmentation is time-consuming, and a fast and reproducible method to approximate right ventricular sinus function would be beneficial.
Tricuspid annular plane systolic excursion is a commonly used objective method of estimating right ventricular function. Tricuspid annular plane systolic excursion can be performed on images from either echocardiography or cardiac MRI. Although cardiac MRI has decreased temporal resolution, it provides excellent spatial resolution, and cardiac MRI tricuspid annular plane systolic excursion correlates well with tricuspid annular plane systolic excursion measured by echocardiography.Reference Kaul, Tei, Hopkins and Shah 3 – Reference Koestenberger, Ravekes and Nagel 6 Tricuspid annular plane systolic excursion validation in children and adults with repaired tetralogy of Fallot has revealed disappointing results.Reference Koestenberger, Nagel and Ravekes 7 – Reference Bonnemains, Stos, Vaugrenard, Marie, Odille and Boudjemline 10 We hypothesised that the poor correlation between tricuspid annular plane systolic excursion and right ventricular ejection fraction in repaired tetralogy of Fallot patients is due to aneurysmal dilatation of the right ventricular outflow tract and that the tricuspid annular plane systolic excursion may be a surrogate for right ventricular sinus ejection fraction.
Materials and methods
Patient population
This cross-sectional, retrospective study was approved by the Institutional Review Board. Patients with repaired tetralogy of Fallot who underwent cardiac MRI between 2007 and 2012 were identified from the cardiac MRI database. The first available cardiac MRI was used if patients had undergone multiple MRIs. Exclusion criteria were the following: over 18 years of age at time of MRI, poor image quality, tricuspid regurgitation greater than moderate, and original anatomy of pulmonary atresia or isolated pulmonary stenosis.
Image acquisition
Images were obtained on either a 1.5-Tesla Siemens Avanto (Siemens Healthcare Sector, Erlangen, Germany) or a 1.5-Tesla Philips Intera (Philips Medical Systems, Best, The Netherlands) using a standard imaging protocol.Reference Schulz-Menger, Bluemke and Bremerich 11 Steady-state free precession sequences were obtained in a short-axis stack. Typical imaging parameters were as follows: slice thickness 8 mm, no gap, field of view 360×360 mm, matrix 208×256, spatial resolution <2.2×2.0×8 mm, flip angle 80°, temporal resolution<55 ms, and minimum echo time and repetition time; the sequences were breath-holds, the cardiac gating was retrospective, and parallel imaging with GRAPPA (Siemens Healthcare Sector) and SENSE (Philips Medical Systems) with an acceleration factor of 2 was used.
Image analysis
Right ventricular volume and ejection fraction were calculated with manual contouring of the endocardial borders in end diastole and end systole using the Leonardo Workstation (Siemens Healthcare Sector) or Diagnosoft Virtue (Diagnosoft, Durham, North Carolina, United States of America). Cardiac MRI tricuspid annular plane systolic excursion was measured by three observers – J.S., E.U., and D.P. – in repaired tetralogy of Fallot patients as described previously (Fig 1).Reference Nijveldt, Germans, McCann, Beek and van Rossum 5 , Reference Caudron, Fares, Vivier, Lefebvre, Petitjean and Dacher 12 The distance from the tricuspid annulus to the right ventricular apex in systole (D2) was subtracted from the distance from the tricuspid annulus to the right ventricular apex in diastole (D1). In order to account for differences in body size in children, the tricuspid annular plane systolic excursion was indexed to body surface area. A fractional tricuspid annular plane systolic excursion was also calculated using the following equation:
 $${{{\rm D}1{\minus}{\rm D}2} \over {{\rm D}1}}$$
$${{{\rm D}1{\minus}{\rm D}2} \over {{\rm D}1}}$$
In addition, tricuspid annular plane systolic excursion measurements were assigned a Z-score based on published values for age.Reference Koestenberger, Ravekes and Everett 13
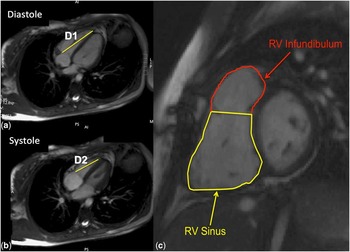
Figure 1 ( a and b ) Tricuspid annular plane systolic excursion was calculated by subtracting the distance from the tricuspid annulus to the apex in systole (D2) from the same distance in diastole (D1). ( c ) RV segmentation in patients with tetralogy of Fallot. The septal and parietal bands were used to divide the right ventricle into the sinus and infundibular portions. RV=right ventricle.
Right ventricular segmentation was performed in the repaired tetralogy of Fallot patients as described by Kutty et al.Reference Kutty, Zhou, Gauvreau, Trincado, Powell and Geva 2 Using the septal and parietal bands, the right ventricle was divided into the sinus and infundibular portions (Fig 1) and then manually contoured. This allowed for the calculation of right ventricular infundibular and sinus volumes and ejection fractions. These measurements were performed by a single observer (J.S.) with a random sample of 24 contoured by a second observer (D.P.).
Statistical analysis
Agreement between readers was assessed using intra-class correlation coefficients. The mean tricuspid annular plane systolic excursion measurements from all the readers were obtained and used to calculate the average, indexed, and fractional tricuspid annular plane systolic excursion measurements. The correlations between the measures of tricuspid annular plane systolic excursion and global and segmental right ventricular function were assessed using the Spearman correlation. Statistical analysis was performed using SPSS 21 (IBM, Armonk, New York, United States of America).
Results
A total of 87 patients were identified, and 54 met inclusion and exclusion criteria. The majority of cardiac MRIs were performed on the Siemens scanner (n=46). Demographics of the patients are listed in Table 1. The most common palliative surgery was a right Blalock–Taussig shunt. The majority of patients had a history of transannular patch repair.
Table 1 Demographics.

RVEDV=right ventricular end-diastolic volume; RVEF=right ventricular ejection fraction; RVESV=right ventricular end-systolic volume; RV-PA=right ventricular to pulmonary artery conduit
Cardiac MRI tricuspid annular plane systolic excursion measurements had good agreement between all three observers (Table 2). Right ventricular segmentation in repaired tetralogy of Fallot patients had good agreement for the right ventricular sinus but only adequate agreement for the right ventricular infundibulum. Table 3 lists the cardiac MRI tricuspid annular plane systolic excursion values obtained for the cohort.
Table 2 Inter-observer variability of TAPSE measurements and right ventricular segmentation using ICC coefficient.

ICC=intraclass correlation; RVEDVinfundibulum=right ventricular infundibular end-diastolic volume; RVESVsinus=right ventricular sinus end-systolic volume; RVEDVsinus right ventricular sinus end-diastolic volume; RVESVinfundibulum=right ventricular infundibular end-systolic volume; TAPSE=tricuspid annular plane systolic excursion
Table 3 Mean TAPSE values.

TAPSE=tricuspid annular plane systolic excursion
Correlations are shown in Table 4. The brand of the MRI scanner did not appreciably affect the correlations. Tricuspid annular plane systolic excursion did not correlate significantly with global right ventricular ejection fraction (r=0.23, p=0.099), although it did correlate weakly with the right ventricular end-diastolic volume (r=0.29, p=0.034). The indexed tricuspid annular plane systolic excursion also had no correlation with global right ventricular ejection fraction and had only weak correlation with the indexed right ventricular end-diastolic volume (r=0.34, p=0.011). Fractional tricuspid annular plane systolic excursion had a weak correlation with global right ventricular ejection fraction (r=0.41, p=0.002).
Table 4 Correlation between TAPSE measurements and measures of right ventricular global and segmental size and function.

RV infundibular EF=right ventricular infundibular ejection fraction; RV sinus EF=right ventricular sinus ejection fraction; RVEDV=right ventricular end-diastolic volume; RVEDVinfundibulum=right ventricular infundibular end-diastolic volume; RVEDVsinus=right ventricular sinus end-diastolic volume; RVEF=right ventricular ejection fraction; RVESV=right ventricular end-systolic volume; RVESVinfundibulum=right ventricular infundibular end-systolic volume; RVESVsinus=right ventricular sinus end-systolic volume; TAPSE=tricuspid annular plane systolic excursion
Evaluated using the Spearman correlation
Tricuspid annular plane systolic excursion and indexed tricuspid annular plane systolic excursion did not correlate with the right ventricular sinus ejection fraction – r=0.24, p=0.076 and r=−0.01, p=0.950, respectively. Fractional tricuspid annular plane systolic excursion, however, correlated weakly with the right ventricular sinus ejection fraction (r=0.3, p=0.028) (Fig 2). Indexed tricuspid annular plane systolic excursion correlated weakly with the indexed right ventricular sinus end-diastolic volume (r=0.36, p=0.007), and fractional tricuspid annular plane systolic excursion correlated weakly with the indexed right ventricular sinus end-systolic volume (r=−0.36, p=0.008). Otherwise, the correlations between measures of cardiac MRI tricuspid annular plane systolic excursion and segmental right ventricular chamber sizes were not significant.

Figure 2 Scatterplots demonstrate ( a ) no correlation between cardiac MRI TAPSE and RV sinus EF, ( b ) no correlation between indexed cardiac MRI TAPSE and RV sinus EF, and ( c ) poor correlation between fractional cardiac MRI TAPSE and RV sinus EF. EF=ejection fraction; RV=right ventricle; TAPSE=tricuspid annular plane systolic excursion.
Tricuspid annular plane systolic excursion Z-scores were calculated based on published values for age. There was a weak correlation between tricuspid annular plane systolic excursion Z-scores and both global and right ventricular sinus ejection fractions – r=0.3, p=0.027 and r=0.31, p=0.021, respectively. Patients were dichotomised to either normal tricuspid annular plane systolic excursion (Z-score of >−2) or abnormal tricuspid annular plane systolic excursion (Z-score of ⩽−2). This dichotomisation was unable to adequately differentiate between patients with normal and abnormal right ventricular function by cardiac MRI (Fig 3).
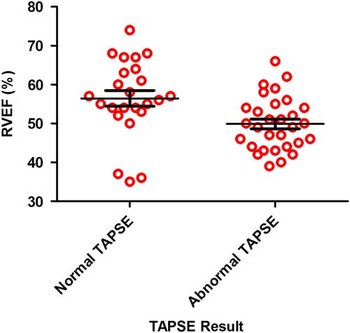
Figure 3 Scatterplot comparing RVEF in patients with normal and abnormal TAPSE based on paediatric Z-scores demonstrates significant overlap between groups. RVEF=right ventricular ejection fraction; TAPSE=tricuspid annular plane systolic excursion.
Discussion
We demonstrated that the measurement of tricuspid annular plane systolic excursion by cardiac MRI is reproducible but correlates poorly with global right ventricular ejection fraction and right ventricular sinus ejection fraction in children with repaired tetralogy of Fallot. These negative results hold true for indexed tricuspid annular plane systolic excursion and fractional tricuspid annular plane systolic excursion – two different methods of accounting for varying patient size in paediatric populations. This is clinically significant because multiple investigators use tricuspid annular plane systolic excursion to estimate right ventricular function with both echocardiography and cardiac MRI. These data suggest that cardiac MRI tricuspid annular plane systolic excursion is a poor surrogate of global or segmental right ventricular ejection fraction in patients with repaired tetralogy of Fallot.
The poor correlation between tricuspid annular plane systolic excursion and global right ventricular ejection fraction has been reported in other studies.Reference Mercer-Rosa, Parnell, Forfia, Yang, Goldmuntz and Kawut 8 – Reference Bonnemains, Stos, Vaugrenard, Marie, Odille and Boudjemline 10 This is likely secondary to the complex right ventricular geometry and right ventricular outflow tract aneurysmal dilatation. The poor correlation with segmental function, however, is more difficult to explain. It may be related to the complex mechanics of right ventricular contraction. Although many studies have demonstrated the importance of longitudinal contraction in assessing right ventricular function,Reference Brown, Raina, Katz, Szerlip, Wiegers and Forfia 14 a recent analysis demonstrated that transverse contraction correlated more strongly with right ventricular ejection fraction than tricuspid annular plane systolic excursion in adults with pulmonary hypertension.Reference Kind, Mauritz, Marcus, van de Veerdonk, Westerhof and Vonk-Noordegraaf 15 In addition, tricuspid annular plane systolic excursion represents longitudinal wall motion along one plane in the right ventricle and cannot account for segmental wall motion abnormalities, which are frequently present in patients with repaired tetralogy of Fallot.Reference Vogel, Sponring, Cullen, Deanfield and Redington 16
The poor correlation also may be related to the varying size in children. We corrected for this by indexing the cardiac MRI tricuspid annular plane systolic excursion, using a fractional cardiac MRI tricuspid annular plane systolic excursion, and by using previously published Z-scores, but it is possible that these are sub-optimal correction methods. Tricuspid annular plane systolic excursion may also reflect left ventricular function, thus decreasing its specificity for, and correlation with, right ventricular ejection fraction.Reference Lopez-Candales, Rajagopalan, Saxena, Gulyasy, Edelman and Bazaz 17 , Reference Lamia, Teboul, Monnet, Richard and Chemla 18 A better method for evaluating global longitudinal contraction, such as strain or strain rate, may provide a better correlation.
Although tricuspid annular plane systolic excursion measured by cardiac MRI may provide data regarding longitudinal motion, our study suggests that these tricuspid annular plane systolic excursion values are not estimates of global or segmental right ventricular ejection fraction in children with repaired tetralogy of Fallot. This should be taken into consideration when interpreting cardiac MRI tricuspid annular plane systolic excursion values. In addition, given the good correlation reported between cardiac MRI tricuspid annular plane systolic excursion and echocardiographic tricuspid annular plane systolic excursion, this study questions the utility of tricuspid annular plane systolic excursion in repaired tetralogy of Fallot patients using either modality.
Limitations
Although cardiac MRI has decreased temporal resolution, it provides excellent spatial resolution, and cardiac MRI tricuspid annular plane systolic excursion correlates well with tricuspid annular plane systolic excursion measured by echocardiography.Reference Koestenberger, Ravekes and Nagel 6 In addition, cardiac MRI tricuspid annular plane systolic excursion has the advantage of being performed at nearly the same time as right ventricular ejection fraction, minimising any differences in right ventricular function caused by changes in pre-load or afterload. Therefore, cardiac MRI tricuspid annular plane systolic excursion has the potential to demonstrate better correlation with right ventricular ejection fraction than echocardiographic tricuspid annular plane systolic excursion. Although it is possible that the relationship between tricuspid annular plane systolic excursion and right ventricular ejection fraction is non-linear, a non-linear relationship should also be detected using the Spearman correlation. Tricuspid annular plane systolic excursion in this study was measured from the annulus to the apex, which is the standard measurement performed in previous cardiac MRI studies.
Conclusions
Cardiac MRI tricuspid annular plane systolic excursion has poor correlation with global and segmental right ventricular ejection fraction in children with repaired tetralogy of Fallot.
Acknowledgement
None.
Financial Support
The project was supported by the National Center for Research Resources, Grant UL1 RR024975-01, and is now supported by the National Center for Advancing Translational Sciences, Grant 2 UL1 TR000445-06. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Conflicts of Interest
None.
Ethical Standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the Belmont report and with the Helsinki Declaration of 1975, as revised in 2008, and has been approved by the Vanderbilt Institutional Review Board.







