


Case report
A term male neonate was born at 39 weeks of gestation by elective Caesarean section under general anaesthesia to a healthy 25-year-old woman with adequate prenatal care and unremarkable prenatal structural ultrasounds. Immediately following delivery, the patient became apnoeic and required immediate resuscitation including chest compressions. He was transferred to the neonatal ICU for further stabilisation and was emergently intubated for agonal breathing with respiratory acidosis.
Notably, the neonatology team reported the presence of stridor despite satisfactory position of the endotracheal tube. The remainder of the physical examination was otherwise unrevealing. An echocardiogram was requested to rule out severe pulmonary hypertension and any other structural cardiac problems. The sonographer raised the concern of hypoplastic aortic arch with severe coarctation of the aorta and immediately informed the cardiology team for confirmation. A small transverse aortic arch was seen in the images that were obtained, but there was a conspicuous absence of right heart dilatation, and intra-cardiac anatomy was normal. Additional focused aortic arch imaging revealed findings of a double aortic arch with a right dominant aorta, and a diminutive left aortic arch (Fig 1; Supplementary video). Both the arches were shown to connect to the descending aorta by two dimension and colour Doppler imaging.

Figure 1 Suprasternal aortic arch imaging performed in the longitudinal plane with a leftward sweep commencing at the superior caval vein. The dominant right aorta is demonstrated (top panel). Following a continued sweep through the endotracheal tube, the hypoplastic left aortic arch becomes apparent (bottom panel, white arrow).
Prolonged need for ventilator support and stridulous breath sounds despite endotracheal intubation raised a suspicion of airway obstruction. Although double aortic arch was already suspected by echocardiogram, given the rarity of acute severe airway obstruction from double aortic arch in the early neonatal period, bronchoscopy was initially performed to rule out any other confounding aetiologies for the obstruction. The bronchoscopy showed pulsating airway compression just distal to the tip of the endotracheal tube (which should be consistent with the extrinsic compression from the vascular ring), but the procedure was terminated before full assessment of the airway could be obtained owing to poor patient tolerance. A CT angiogram of the chest was performed, which confirmed the presence of a double aortic arch with right-sided dominance (Fig 2). Dynamic airway evaluation by CT was performed by slightly withdrawing the endotracheal tube, which confirmed severe tracheal compression at the site of the vascular ring with no other major associated airway abnormalities (Fig 3; Supplementary videos).
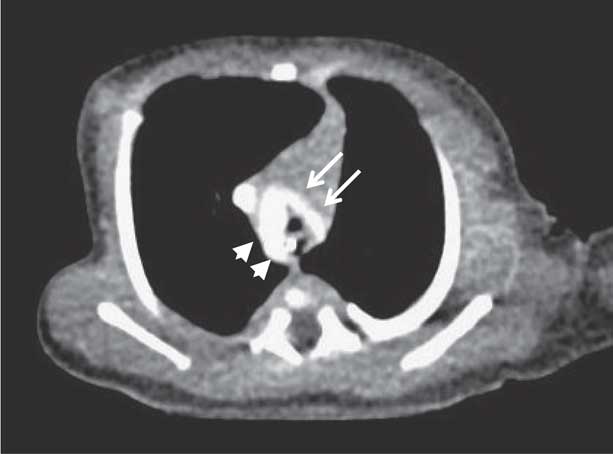
Figure 2 Axial image of double aortic arch with right-sided dominance on CT angiogram (arrowheads). The diminutive left-sided arch is shown (white arrows).
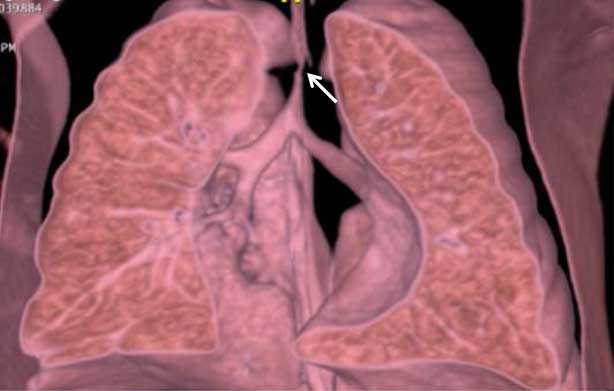
Figure 3 Respiratory assessment using dynamic airway evaluation on CT imaging demonstrates the presence of significant and severe tracheal stenosis due to compression from the vascular ring. The diameter of the trachea narrows to 2 mm at the site of compression (white arrow).
The patient ultimately underwent surgical division of the hypoplastic left aortic arch and the ductus arteriosus ligament via a left posterolateral thoracotomy incision. He was extubated on the 1st post-operative day. His post-operative course was complicated by anticipated tracheomalacia, which required non-invasive positive pressure ventilation for a few days. He slowly improved with conservative measures and was ultimately discharged home.
Discussion
Double aortic arch is the most common type of vascular ring anomaly that typically manifests in infancy or early childhood with symptoms of tracheal and/or oesophageal compression.Reference Backer, Mongé, Popescu, Eltayeb, Rastatter and Rigsby 1 Respiratory symptoms include cough, dyspnoea, recurrent pulmonary infections, stridor, and respiratory distress with feeds.Reference Griswold and Young 2 Symptoms due to oesophageal compression, namely dysphagia and choking and feeding intolerance, can arise as early as the 1st year of life but usually become apparent during childhood. Although uncommon, double aortic arch can be diagnosed well into adulthood. In general, older children and adults typically present with symptoms related to oesophageal compression more commonly than respiratory symptoms. Although respiratory symptoms are reported in the neonatal period, critical tracheal compression leading to respiratory failure immediately after birth is a rare manifestation of double aortic arch.Reference Moon, Mayor and Younis 3 – Reference Cannioto, Ngalikpima and Dall’Amico 5 Nevertheless, this can provide a diagnostic and therapeutic dilemma, owing to a widely held and generally correct notion that respiratory failure is not a typical manifestation of the disease in the immediate neonatal period. In one series of 81 children, surgical repair was necessary at a median age of 6 months, with the youngest patient repaired at 3 days of life.Reference Alsenaidi 6 Severe respiratory compromise has even been reported as early as fetal life, as highlighted in one case of vascular ring with a right dominant double aortic arch.Reference Shum 7 A strong index of suspicion is necessary.
Echocardiographic evaluation of any patients with suspected airway/oesophageal obstruction should always include the assessment of aortic arch anatomy, arch sidedness, and head and neck vessel branching pattern. In double aortic arch, the right arch is usually (72%) dominant, with the left arch commonly being hypoplastic.Reference Alsenaidi 6 On routine echocardiographic technique (optimal for imaging the left aortic arch) one could potentially visualise the hypoplastic left arch and miss the dominant right arch that might lead to the false impression of hypoplastic aortic arch or coarctation of aorta as described in this case. The presence of hypoplastic aortic arch without any other echocardiographic evidence of arch obstruction (e.g. right heart dilation) should lead to the suspicion for double aortic arch prompting one to look for the dominant right arch.
The decision to proceed to surgical intervention was based on judicious diagnostic workup and the ability to demonstrate the tracheal compression and stenosis due to the vascular ring by dynamic airway evaluation on CT imaging. The dynamic CT airway evaluation was helpful in identifying the degree of associated airway abnormalities (such as tracheomalacia) and ruling out other possibilities of airway compromise. The degree of tracheomalacia did not appear severe enough by dynamic airway evaluation to warrant surgical intervention specific to the airway; therefore, the surgical planning was primarily directed at alleviating the vascular ring. A few case reports are available that demonstrate the utility of dynamic airway evaluation in the diagnosis and management of tracheal compression in infants with vascular ring anomalies.Reference Rogalla, Wauer and Rogalla 8 – Reference Gaafar and El-Noueam 10 With current dose modulation techniques, the radiation exposure for dynamic airway evaluation can be reduced to as low as reasonably achievable and results in effective radiation doses that are not much higher than a regular chest CT, as was the case in our patient. In conclusion, we believe that an advanced imaging modality such as CT with dynamic airway evaluation provides valuable information in neonates with evidence of critical respiratory compromise from vascular rings, including double aortic arch.
Acknowledgements
The authors would like to thank the reviewers whose comments and suggestions helped improve this manuscript. We also wish to thank Drs. Jeffrey Scrugham and Jason N. Johnson for their assistance in performing and interpreting the patient's chest CT.
Financial Support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflicts of Interest
None.
Ethical Standards
None.
Supplementary Material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1047951117002335





