



Kawasaki disease is a disease known to cause a spectrum of coronary abnormalities ranging from simple dilation to giant aneurysm and rupture. Dilation is typically seen extreme 4–6 weeks after diagnosis. It can either remain unchanged or progress further, develop thrombosis, and ultimately coronary insufficiency among patients with coronary aneurysm. Reference McCrindle, Rowley and Newburger1 Due to these long-term complications, serial assessment of the coronary arteries is important after aneurysm is initially detected.
Most commonly serial assessment is via echocardiography; however, echocardiography is operator dependent, and visualisation of distal coronary lesions can be challenging. Echocardiography alone is sometimes insufficient for evaluation of progression of coronary aneurysm. Reference Xing, Wang, Yu, Chen and Hou2 Multi-detector CT technology has been an accepted non-invasive imaging tool to assess coronary arteries in adults. However, its utilisation in children is limited by their higher heart rates, inability to breath-hold, and to follow instruction. Furthermore, there is no standard protocol for younger children. Nevertheless, with the new generation of dual source, higher gantry rotation and slices, small coronary structures can be depicted clearly using an electrocardiogram triggered protocol. Reference Achenbach, Marwan and Schepis3,Reference Husmann, Leschka and Desbiolles4 Moreover, radiation dose can be minimised. The typical effective dose for chest CT is 5–8 millisievert, and doses of 10 millisievert are needed for coronary assessment. Reference Goo5
In our institution, we have performed CT coronary angiogram in selected Kawasaki patients with coronary aneurysm diagnosed or suspect on echocardiogram since 2014. Here, we report our initial experience in these patients. Emphasising techniques of image acquisition and seeking to assess the diagnostic quality, the effect of heart rate on the image quality and the effective radiation dose involved in the study.
Material and methods
Patients
This is a retrospective study involving post Kawasaki patients up to 18 years diagnosed to have coronary aneurysm or suspected to have coronary stenosis on echocardiogram referred for CT coronary angiogram between 27th February, 2014 and 17th May, 2017. Demographic data, CT coronary angiogram protocol, vital signs, coronary CT images and radiation dose were evaluated.
Multi-detector CT protocol
All studies were performed using a 64-slice dual source CT scanner (Somaton by Siemen) with strict adherence to As Low as Reasonably Achievable “ALARA” principles. We used Iomeron 350 contrast with minimum 20 ml of saline push depending on patient’s weight. The imaging protocol was tailored based on patients’ cooperation and heart rate. Breath holding protocol was used in a cooperative patient, while in those unable to cooperate, the study was performed under general anaesthesia (using a short-acting muscle relaxant by anaesthetist). We used right ventricle as region of interest during image acquisition. Retrospective electrocardiogram-gated protocol was used in those with heart rate of more than 70 beats per minute, and prospective electrocardiogram-gated protocol was used in those with heart rate of less than 70 beats per minute (as in adult protocol). Reference Husmann, Leschka and Desbiolles4 The scanning was performed regardless patient’s heart rate at either 80 or 100 kilovoltage peak for patients who weigh less than 20 and more than 20 kg, respectively. We did not routinely use beta-blockers to reduce heart rate to avoid hypotension. Patient’s heart rate, SaO2, and blood pressure were continuously monitored throughout the procedure. Contrast of 1–2 mg/kg was given via an injector at the highest flow rate tested for the size of cannula before the study. Any procedure-related complications (e.g. skin rash, hypotension, extravasation, etc.) and radiation parameters (scanning time and dose-length product) were recorded.
Post-processing analysis
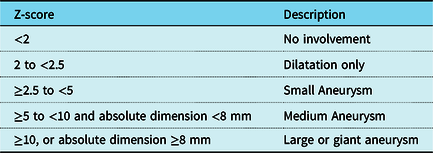
The coronary arteries were evaluated for the presence of aneurysms, stenosis, thrombus or total occlusion by a consultant paediatric cardiologist and an adult consultant cardiac imaging cardiologist that performed this study. The image quality of the coronary artery (left main, left anterior descending, left circumflex, and right coronary artery) was determined based on a 5-grade scoring system (5, clearly visible without motion artefacts; 4, mild motion artefacts but coronary course readily traced; 3, substantial blurring, but initial coronary course traceable, and sufficient to exclude an abnormal coronary course before surgery; 2, coronary artery course uncertain; 1, no coronary segments identified). This scoring system was adapted from Paul et al. Reference Paul, Rohnean, Elfassy and Sigal-Cinqualbre6 In this interpretation, Grades 4 and 5 are considered as excellent, whereas grades 3, 2, and 1 are tabulated as good, satisfactory, and poor, respectively. Classification of coronary artery dilatation is based on Z-score as shown in Table 1, which is based on recommendations from the American Heart Association (Diagnosis, treatment, and long-term management of Kawasaki Disease 2017 guideline). Reference McCrindle, Rowley and Newburger1 The effective radiation dose in millisievert was calculated using dose length product x age- and sex-specific conversion factors as published by Goo. Reference Goo5
Table 1. Coronary artery dilation based on Z score (AHA diagnosis, treatment and long-term management of Kawasaki Disease 2017 guideline).
Statistical analysis
Patients’ demographic data and radiation dose are expressed in median and range. The association of image quality and heart rate and mean effective was evaluated using Kruskal–Wallis statistical analysis. Fisher exact test was used for other cofounder factors namely between image quality and imaging protocol and kilovoltage peak. p value of less than 0.05 was considered significant.
Results
Demographic
A total of 52 Kawasaki patients underwent CT coronary angiogram to assess coronary artery lesions. The median age was 5 years (range 1–18 years). The median patient weight was 18.2 kg (range 8.2–75.2 kg). During image acquisition, the median heart rate was 88 (range 50–165) beats per minute, as per shown in Table 2. The study was performed under general anaesthesia in 44 patients and breath-holding technique in 9 patients. In patients requiring general anaesthesia, propofol was the drugs of choice followed by ketamine and fentanyl.
Table 2. Patient demographic, and radiation dose parameters.

Radiation parameters and image acquisition protocol
Patients’ radiation parameters are summarised in Table 2. The measured median dose-length product was 57.5 (range 29.2–560.00) milligray and median effective dose of 0.81 (range 0.4–5.8) millisievert. In 42 (80%) patients, the study was performed using end-systolic retrospective triggering protocol, and the rest had end diastolic prospective protocol. Tube length voltage was adjusted to patients’ weight as per recommended where patients with weight < 20 kg used 80 kilovoltage peak (in 45 patients) and for those weighing > 20 kg, we used 100 kilovoltage peak (in 7 patients). Reference Fukazawa, Kobayashi and Ayusawa7,Reference Kuettner, Gehann and Spolnik8
Coronary lesions
Coronary artery lesions were found in 25 (48%) patients. Of these, 19 (76%) had unilateral and 6 had bilateral coronary aneurysms. The lesions were further divided into single and multiple aneurysms in each coronary (Fig 1).

Figure 1. Distribution of coronary artery abnormalities.
In the unilateral aneurysm group, 13 (68%) and 6 (32%) patients has single and multiple aneurysms, respectively. Six of 13 patients with single aneurysm had thrombosis with partial occlusion and one developed thrombosis with total occlusion. While in the multiple aneurysms group, 2 had stenosis and none had thrombosis.
In the bilateral aneurysm group, five of six patients had multiple aneurysms and one had single aneurysm with thrombosis resulting in partial occlusion. Four out of the five patients with multiple aneurysms had thrombosis and among them two had partial occlusion and another two had total occlusion. Figure 2 shows a patient with bilateral, multiple coronary aneurysms complicated with thrombosis resulting in total occlusion of the left anterior descending and partial occlusion of right coronary artery.

Figure 2. Coronary aneurysm in Kawasaki patient. 5 year old child with typical Kawasaki disease; 3.5 years post second Kawasaki with bilateral giant aneurysm with thrombus in LCA. During time of acquisition, heart rate was 70 beats per minute which yield excellent image quality. ( a ) MPR images on 2 giant fusiform aneurysms in proximal (14 × 12 mm) and mid RCA and small saccular aneurysm in distal RCA. ( b ) Cross-section of proximal RCA aneurysm with large thrombus with partial luminal occlusion. ( c ) MIP image on total occlusion of proximal LAD (arrow), small mid and distal LAD with retrograde filling. ( d ) VRT image on small aneurysm of distal RCA (arrow). Distal RCA continues with distal LAD suggesting of retrograde supply to LAD.
Image quality and association with heart rate and radiation dose
The coronary images were graded as excellent in 34 patients (65%), good in 17 (32%) and satisfactory in 1 (2%). None of the images were graded as poor quality (i.e. severe motion artefacts or under-visualised coronary segments).
The heart rate was sub-categorised into four groups namely <80, 80–90, 91–100 and >100 beats per minute. Patients with heart rates greater than 100 beats per minute had significant worse image quality to those with lower heart rates (p = 0.007, Table 3). We also found no association between effective radiation dose and image quality (Table 4).
Table 3. Correlation of heart rate with image quality of the coronary segments.

Table 4. Correlation of effective radiation dose with image quality of the coronary segments.

Discussion
Our study showed either electrocardiogram-triggered prospective or retrospective CT coronary angiography provides a good diagnostic quality evaluation of coronary lesions in children post Kawasaki disease. Patients with heart rate less 100 beats per minute yielded excellent image quality but with lower quality imaging in patients with higher heart rates.
Xing et al emphasised the superiority of CT in detecting coronary artery injury in Kawasaki disease with detection of left coronary artery dilation of 25% compared to transthoracic echocardiography of only 18.8%. The pathology and calcification of the coronary artery is better delineated on CT especially in the mid-distal left anterior descending branch. Reference Xing, Wang, Yu, Chen and Hou2,Reference Nie, Wang, Cheng, Ji, Duan and Chen9 A study done by van Stijn et al in 2019 also showed detection of aneurysm, calcification, plaque and/or thrombi in left circumflex coronary artery was always visible on computed tomography which was not detected on transthoracic echocardiography. Calcification were as early as 2.7 years after onset of disease. Reference van Stijn, Planken, Groenink, Streekstra, Kuijpers and Kuipers10 By comparing with our study, we can further categorise the patients into single or bilateral involvement and further subdivide into number of aneurysms in mid or distal coronary artery. Our study demonstrates that detailed delineation of distal coronaries is feasible on CT. This will be beneficial in deciding on subsequent surveillance for the patients and further mode of investigation for the patient.
The radiation hazards have always been the issue of concern in patients requiring repeated imaging studies and CT represents the most important source of ionising radiation from medical exposure. Children are especially vulnerable to the harmful effects of ionising radiation due to the greater sensitivity of growing tissue and a longer anticipated lifetime to manifest radia
tion induced damage as compared with adults. 11 The risk of radiation in neonatal period is liken to antenatal exposure to radiation. Hence, various strategies to reduce radiation have been proposed. Among this method is prospective electrocardiogram-triggered scanning method is accepted as one of the most effective dose-saving strategies, leading to an approximately 70% reduction of radiation dose compared with retrospective electrocardiogram-gated helical scanning, while still offering comparable imaging quality and diagnostic accuracy. Reference Sun and Ng12 The usage of dual source CT scan has made prospective electrocardiogram-gated scanning more accessible. This scanner provides a temporal resolution of 83 ms, hence shorter exposure to radiation. Reference Stolzmann, Scheffel and Schertle13 Stolzmann et al study showed radiation exposure of dual-source CT coronary angiography using an electrocardiogram-pulsing protocol reducing the tube current to 20% significantly decreases with increasing heart rate. Cardiac catheterisation has always been a gold standard as it would confer both diagnostic and therapeutic value. Study done among patients who underwent radio diagnostic procedure in particular coronary angiogram in 2003 showed radiation doses range between 5.6 and 100 millisievert. Reference Stolzmann, Scheffel and Schertle13 This vast range of radiation exposure might be due to the inclusion of therapeutic procedure. Another aspect of reducing the radiation exposure is reducing the tube voltage to 80 kilovoltage peak and adaptation of the tube current to the infant’s weight. Saad et al Reference Saad, Rohnean, Sigal-Cinqualbre, Adler and Paul14 noted the use of 80 kilovoltage peak setting reduces the need for high contrast medium injection rates or concentration since a low kilovoltage is more sensitive to contrast medium protocol using 80 kilovoltage peak increase sensitivity to contrast medium by 50% compared with 120 kilovoltage peak acquisition.
The American Heart Association guidelines 2018 recommend risk stratification according to Z score (coronary artery diameter corrected for body surface area). The maximal Z score combined with the evolution over time (based on echocardiographic findings) has predictive value for the development of myocardial ischaemia and infarction. Reference McCrindle, Rowley and Newburger1 This predictive value was also in-line with Japanese Kawasaki Guideline 2020. Reference Fukazawa, Kobayashi and Ayusawa7 Hence, CT coronary will be an indispensable tool for surveillance of disease before subjecting patient for further assessment, that is, myocardial perfusion imaging and coronary angiogram.
Our experience showed electrocardiogram-triggered CT coronary angiogram with a heart rate less than 100 beats per minute yields excellent image quality. In our cohort of patients, heart rate was the only factor that affected image quality although with a narrow range of effective dose in our cohort of patients. This can guide us during the procedure in terms of achieving a certain level of heart rate before proceeding with scans, provided haemodynamically safe. On the other note, it was possible to achieve an overall diagnostic image quality in 97% of the examination using a low-dose protocol. CT coronary angiogram also provides a satisfactory assessment of each coronary in children with Kawasaki disease even with median low-dose radiation of 0.7 mSev. There is no standard dose or protocol for beta-blocker administration as preconditioning in children undergoing coronary CT angiography. Watanabe et al in 2018 showed that there was no difference in terms of radiation exposure between those who received beta blocker, and there was no adverse effect. His studies showed that it is safe to use beta blocker namely either short-acting oral beta blocker (0.8 mg/kg/dose) 1 hour before the procedure with additional either oral or intravenous beta blocker during the procedure to achieve the desired heart rate as long patient is haemodynamically stable. Reference Watanabe, Kamiyama, Kato, Komori, Abe and Ayusawa15
Limitations
Identified study limitation is it is a retrospective study with limited sample size. It was also not design to compare other protocols. Hence, we are unable to give more comprehensive conclusion regarding the optimal settings and strategy regarding coronary artery images acquisition. We have also identified the following issues:
-
1. Low volume of patients requiring CT coronary in children resulting in a steep learning curve for radiographers and cardiologist. In our institution, CT coronary study for children is only scheduled once a month for patients requiring anaesthetist support.
-
2. Variability in patients’ size, cooperability, and heart rates makes it difficult to apply standard protocol to every patient. There is no reference on standard protocol available. Hence, the protocol used is based on previous experience of a good-quality image. The result of the same protocol may or may not be reproducible.
-
3. Heart rate is difficult to control in children. The sudden increase in heart rate with the voice instruction will affect the pre-plan protocol and image quality. Furthermore, some anaesthetic drugs like ketamine may cause in tachycardia.
-
4. Beta blocker was not used for the concern on adverse side effects like hypotension at the expense of image quality, especially in patients performed under general anaesthesia.
-
5. As score on image quality was only done by a single paediatric imaging cardiologist, no interobserver agreement can be performed to improve the personal bias.
Conclusion
Our conclusion is electrocardiogram-synchronised CT coronary angiogram provides a good diagnostic assessment of coronary artery lesions in children with Kawasaki disease. However, more regular and frequent studies need to be performed to improve the skill, experience, and successful CT coronary studies in children in order to develop reliable protocol for this group of patients. Heart rate lowering agent like short-acting beta blocker may improve the image quality of coronary artery in those patients with heart rate of more than 100 beats per minute. With the availability of new generation of high-speed CT, a single beat CT coronary study can be performed without general anaesthesia. However, its effect on image quality is yet to be studied.
Acknowledgements
All persons have made substantial contributions to the research and manuscript.
Financial support
None.
Conflicts of interest
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008, and has been approved by the institutional committee of Institut Jantung Negara, Kuala Lumpur, Malaysia.






