A 4-day-old female infant, during a postnatal check, was noted to have bluish discolouration over the lips with percutaneous oxygen saturation of 70%. She required intubation following an apnoeic episode. Despite being ventilated on 100% oxygen, pulse oxymetry could not be raised above 80%. Hence, a prostaglandin infusion was commenced.
Cardiovascular and respiratory examinations were normal. An electrocardiogram showed right atrial hypertrophy. Chest X-ray showed cardiomegaly. Echocardiography showed a large secundum atrial septal defect with a predominantly right-to-left shunt. The tricuspid valve appeared dysplastic with apical displacement of the septal leaflet resulting and a small hypoplastic right ventricular cavity. A large redundant tissue was noted within the right atrium to be protruding into the right ventricle through the tricuspid valve orifice (Fig 1). A diagnosis of Chiari's network and Ebstein's anomaly with raised pulmonary vascular resistance was made from the severity of tricuspid regurgitation. The prostaglandin infusion was stopped. Attempts were made to reduce her pulmonary vascular resistance with inhaled nitric oxide and adenosine infusion. Her oxygen saturation improved slightly but this was not sustained. On the next day, a repeat echocardiography revealed Chiari network malformation in the right atrium as before, a large right atrium and hypoplastic right ventricle with continued suspicion of Ebstein's anomaly due to displacement of the tricuspid valve septal leaflet attachment (Fig 2). She subsequently made good progress after being extubated and was discharged home on sildenafil and overnight home oxygen.

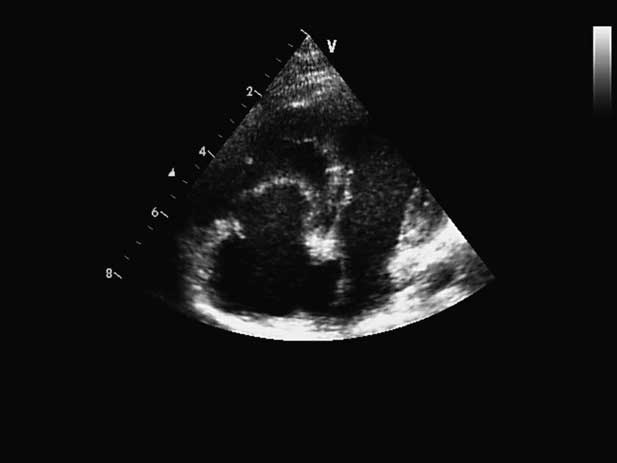
Figure 1 A four-chamber view reveals the floppy membrane of cor triatriatum protruding into the tricuspid valve apparatus and mimicking Ebstein's anomaly.

Figure 2 A four-chamber view shows the redundant membrane (CT), tricuspid valve leaflets (TV), and mitral valve (MV) attachment.
She remained clinically well with percutaneous oxygen saturation of 85% in air. A repeat echocardiogram at 23 months of age showed good-sized right ventricular cavity and increased prominence of Chiari's network. At this time, a redundant venous membrane was noted to be extending from the superior caval vein along the crista terminalis to the mouth of the inferior caval vein and from the inferior caval vein to the foramen ovale. This membrane was subdividing the right atrium into two compartments and resulting in a right-to-left shunt across the atrial septal defect (Fig 3). The diagnosis of cor triatriatum dexter was entertained for the first time on this occasion. The floppy membrane within the right atrium was protruding into the tricuspid valve and pushing the leaflets downwards, giving an impression of Ebstein's anomaly (Fig 4 supplementary AVI file). There was minimal displacement of the septal leaflet with no significant tricuspid regurgitation and good forward flow across the pulmonary valve. The flow through the tricuspid valve was moving on either side of the floppy membrane within the right atrium but there was minimal obstruction.

Figure 3 Cor triatriatum dexter (CT) evident with a membrane subdividing the right atrium (RA) by extending from the SCV to the foramen ovale (FO).
The patient underwent an operation and a clear membrane was identified within the right atrium, which was partially obstructing the tricuspid inlet. This membrane was excised and the ostium secundum defect was closed using an autologous pericardial patch at 28 months of age. She was extubated shortly after admission to the paediatric intensive care unit with normal percutaneous oxygen saturations and was discharged home on day 5. At 2 weeks after surgery, she was well with normal pulse oxymetry measurement. Echocardiogram showed normal intracardiac anatomy mild tricuspid regurgitation with a peak velocity of 2.2 milliseconds suggesting normal right ventricular and pulmonary artery pressures. Right ventricular size was equal to that of the left ventricle.
Discussion
Cor triatriatum dexter or partitioning of the right atrium is a rare congenital anomaly. It is caused by persistence of the right valve of the sinus venosus which divides the right atrium into two chambers: the caval veins and coronary sinus to one side (the sinus venarum) and the tricuspid valve and right atrial appendage on the other (the trabeculated portion).Reference Gussenhoven, Essed and Bos1, Reference Gerlis and Anderson2 The valve usually regresses early during foetal life by the 12th week of gestation, leaving behind the crista terminalis superiorly and the Eustachian valve of the IVC and the thebesian valve of the coronary sinus inferiorly.Reference Gussenhoven, Essed and Bos1 The appearance of the valve can vary from a simple muscle bar to a fenestrated membrane or to Chiari's network as filigreed weblike networks.Reference Trento, Zuberbuhler and Anderson3
Cor triatriatum dexter is frequently associated with important abnormalities of other right cardiac structures including atrial septal defects and Ebstein's anomaly of the tricuspid valve.Reference Gerlis and Anderson2 Cor triatriatum dexter has varying clinical manifestations depending on the degree of partitioning or septation of the right atrium. When the septation is incomplete, the condition is often asymptomatic. It is an incidental finding and the diagnosis is frequently made at a post-mortem examination. More complete septation can cause right-sided cardiac failure and elevated central venous pressures due to obstruction of the tricuspid valve, the right ventricular outflow tract, or the inferior caval vein.Reference Joe and Poustchi-Amin4, Reference Caliskan, Erdogan and Gullu5
In our case, the diagnosis of cor triatriatum dexter became evident with growth of her right ventricle and reduction of pulmonary vascular resistance with the aid of nocturnal home oxygen and sildenafil. The right atrial membrane promoted right-to-left shunting at the atrial level and resulted in cyanosis.Reference Galli, Galletti and Schena6, Reference Mahy and Anderson7 The membrane, by directing part of the venous return of the inferior caval vein into the left atrium and away from the right ventricle, may have contributed to hypoplasia of the right ventricle and reduced pulmonary inflow due to the low flow through the right side of the heart.Reference Trento, Zuberbuhler and Anderson3
The synergistic use of adenosine infusion combined with nitric oxide did not prove beneficial. We postulate that the use of oxygen and sildenafil led to reduction of pulmonary vascular resistance, moderate improvement in oxygen saturation, and increased tricuspid and pulmonary flow with eventual growth and development of the right ventricle. Thus, it was later noted that there was a large membrane within the right atrium, which was protruding towards the right ventricle and pushing the tricuspid leaflets downwards, masquerading as Ebstein's anomaly. A recent report by Barrea et al described a similar case of cor triatriatum dexter mimicking Ebstein's disease.Reference Barrea, Rubay and Wagner8
Owing to its paucity, diagnosis of cor triatriatum dexter can be difficult. In a majority of cases, the right atrial membrane was reportedly found at the operating table or upon autopsy.Reference Gussenhoven, Essed and Bos1 It is important to recognise on time cor triatriatum dexter as it is amenable to simple surgical correction with resection of the right atrial membrane and closure of the atrial septal defect.Reference Erk, Kolbakir and Baysal9 In some cases, owing to high surgical risk, percutaneous balloon dilation of the obstructive membrane may be considered to relieve the atrial obstruction.Reference Savas, Samyn and Schreiber10
This report highlights the difficulties in recognising cor triatriatum dexter. The condition can particularly mimic Ebstein's anomaly or hypoplastic right ventricle in newborn babies and infants.