


A quadricuspid arrangement is a rare congenital malformation of the aortic valve. Most of the published cases have been discovered incidentally at autopsy, aortography, or during surgery for replacement of the valves. In 2 large series investigation autopsied hearts, incidence was reported at 0.003%,Reference Simonds1 and 0.008%.Reference Hurwitz and Roberts2 The malformation is an uncommon cause of aortic regurgitation in adults. In reports of series of patients undergoing surgery for pure aortic regurgitation, the incidence has been estimated at 0.88%,Reference Olson, Subramanian and Edwards3 and 1.46%.Reference Yutsumoto, Iguro, Kinjo, Matsumoto, Masuda and Sakata4 Although the lesion has sometimes been diagnosed in association with other congenital cardiac defects,Reference Janssens, Klues and Hanrath5 few cases have been reported in children. In this article, we describe our experience with 3 children diagnosed with the malformation at our Institution. All had been investigated with clinical examination, electrocardiography, transthoracic echocardiography, and exercise stressing test between October and November, 2007.
Description of the cases
Clinical data, and echocardiographic features, are summarized in Table 1. In all, the diagnosis was made by transthoracic echocardiography using the parasternal short axis view. Our female patient had been referred for the first time for a pre-operative evaluation. On physical examination, she presented an apical click and a late systolic murmur suggestive of mitral valve prolapse. Because of this, she was examined using transthoracic echocardiography. The other 2 children were evaluated initially as outpatients, having been diagnosed previously as having bicuspid aortic valves producing mild aortic regurgitation. All children were asymptomatic. The electrocardiogram was normal in the 2 boys, but our female patient had left axis deviation. In our first patient, a boy aged 6 years, the valve was shown to possess 2 large leaflets of equal size, and 2 smaller leaflets, also of equal size. There were three aortic sinuses, with a raphe separating the two smaller leaflets, both located in the right coronary aortic valvar sinus. (Fig. 1). The second patients, a girl aged 11 years, had a valve with 3 large leaflets of equal size, and 1 smaller leaflet. The small accessory leaflet was placed anteriorly in the left coronary aortic valvar sinus, being separated from the right leaflet and from the wider left leaflet by well delineated zones of apposition (Fig. 2). An associated prolapse of the mitral valve causing trivial regurgitation was documented using the parasternal long axis view. In the third patient, a boy aged 6 years, the valve possessed 4 leaflets of approximately equal size (Fig. 3). Of the leaflets, 2 were located in the right coronary aortic valve sinus. Doppler analysis, combined with colour flow mapping, revealed mild central aortic regurgitation due to incomplete diastolic coaptation of the leaflets in the first and third patients (Fig. 4). The valve was functioning normally in the second patient. In both children with regurgitant valves, measurement of cross-sectional images normalized for body surface area revealed dilation of the aortic rootReference Roman, Devereux, Kramer-Fox, O’Loughlin, Spitzer and Robins6 (Table 2 – Fig. 5). At their last visit to our clinic, all children performed an exercise stress test using a treadmill, maximal in two of them, and showed neither symptoms nor electrocardiographic anomalies during effort.
Table 1 Clinical data and echocardiographic features of children with quadricuspid aortic valve.

m: male; f: female; S.: systolic; LAD: left axis deviation; AR: aortic regurgitation; MVP: mitral valve prolapse.
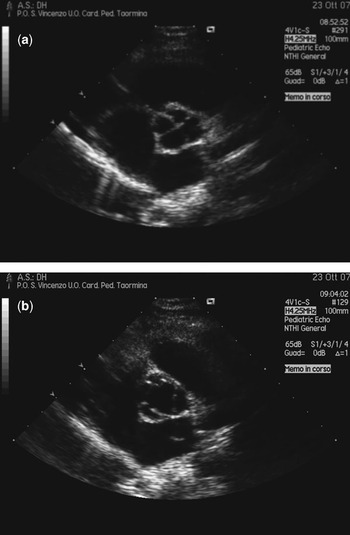
Figure 1 The echocardiographic view (a) in diastole shows a quadricuspid aortic valve with 2 larger and 2 small leaflets in our first patient. The systolic frame (b) shows a raphe between the two smaller leaflets.

Figure 2 In the second child, the valve has 3 leaflets of equal size and 1 smaller leaflet.

Figure 3 The parasternal short axis view in the third child shows an aortic valve with four leaflets of equal size.

Figure 4 Color Doppler interrogation shows central mild aortic regurgitation in the first patient (a). Interrogation in the third child (b) revealed mild aortic regurgitation due to incomplete diastolic coaptation of the leaflets.
Table 2 Measurements of the aortic root from the proximal hinges of the leaflets to the sinutubular junction.

The first and third children show dilation of the aortic root when normalised to body surface area. Both were shown to have mild aortic regurgitation using colour flow analysis.
BSA: body surface area; Prox.: proximal; ST.J: sinotubular junction; As. Ao: ascending aorta; AR: aortic regurgitation.

Figure 5 Measurements in the third child reveal dilation of the aortic root from the proximal hinges of the leaflets to the sinutubular junction and the proximal part of the ascending aorta. The diameter at the hinges of the leaflets is 17 millimeters (measure n.1), the dimension at the midpoint of the sinuses of Valsalva level is 24 millimeters (measure n.2), at the sinutubular junction is 21 millimeters (measure n.3), and the proximal ascending aorta measures 22 millimeters (measure n.4).
Discussion
A quadricuspid arrangement of the aortic valve is rare.Reference Tutarel7 Unlike the quadricuspid pulmonary valve, the quadricuspid aortic valve is often incompetent,Reference Davia, Fenoglio, DeCastro, McAllister and Cheitlin8 with regurgitation being the most common functional abnormality.Reference Timperley, Milner, Marshall and Gilbert9 Hurwitz and RobertsReference Hurwitz and Roberts2 used an alphabetic classification based on the size of the leaflets for categorisation, but we find description of the valvar leaflets and the aortic root to be more meaningful. The anomaly has been diagnosed in association with other congenital anomalies, such as persistent patency of the arterial duct, ventricular septal defect, pulmonary stenosis, mitral valvar malformations, supravalvar aortic stenosis, hypertrophic cardiomyopathy, congenital atrioventricular block and coronary arterial abnormalities.Reference Janssens, Klues and Hanrath5 The most frequent associated anomaly is the displacement of a coronary arterial orifice, which is important to recognize, especially from a surgical standpoint. Indeed, patients with quadricuspid and regurgitant valves often need surgical treatment during adulthood. Although aortic valvoplasty and reduction of the valvar diameter have been attempted, replacement is usually performed in the majority of patients.Reference Yutsumoto, Iguro, Kinjo, Matsumoto, Masuda and Sakata4 In this setting, it is important to recognize any displacement of the coronary arterial orifices in order to prevent obstruction when suturing the ring of the valvar prosthesis.Reference Tutarel10 Only a few cases have been diagnosed incidentally by echocardiography in otherwise asymptomatic children,Reference Coeurderoy, Biron, Laurent and Almange11, Reference Divakaramenon and Venugopal12 albeit that the diagnosis has been made in association with coronary arterial anomalies in children with symptoms of myocardial ischaemia. Kurosawa and colleaguesReference Kurosawa, Wagenaar and Becker13 made the diagnosis at autopsy in a boy aged 16 year who died suddenly, finding 3 leaflets of equal size and one smaller dysplastic leaflet. The additional leaflet was thick and totally adherent to the aortic wall, producing isolation of the main stem of the left coronary artery. In addition, histology revealed disarrangement of the elastin fibres typical of supravalvar aortic stenosis. Isolation of the left coronary artery by 1 leaflet adherent to the aortic wall was also diagnosed in a girl aged 10 year during an emergency operation for an acute myocardial infarction.Reference Mutsuga, Tamaki and Yokoyama14 The anomaly was also found during surgery for coronary arterial orificial atresia in a 5 year old child affected by supravalvar aortic stenosis.Reference Rosenkranz, Murphy and Cosgrove15 In all our patients, the coronary arteries arose in their expected fashion from the aortic sinuses adjacent to the pulmonary trunk. Irrespective of such findings, in view of the reported association with isolation of coronary arteries, we consider it advisable to rule out myocardial ischaemia in all children with quadricuspid valve, at least with non-invasive methods. Because of this, we performed an exercise stress test in all our children, even though they were asymptomatic. It is also important to monitor the degree of aortic regurgitation during follow-up,Reference Barbosa and Motta16 and prophylaxis for infective endocarditis should also be considered.Reference Timperley, Milner, Marshall and Gilbert9, Reference Takeda, Ohtaki, Kasegawa, Tobaru and Sumiyoshi17
The physiopathology of aortic regurgitation is poorly understood. Abnormal shear stress leading to fibrosis, incomplete coaptation of the leaflets, prolapse of the leaflets, or dilation of the aortic root have all been proposed.Reference Godefroid, Colles, Vercauteren, Louagie and Marchandise18 With this in mind, it is of interest that we found dilated aortic roots in 2 of our patients in the setting of mild aortic regurgitation. It is, of course, frequent to find a dilated ascending aorta, independent of the haemodynamic state of the valve, in those with the bifoliate arrangement.Reference Gurvitz, Chang, Drant and Allada19 To the best of our knowledge, ours is the first report of such dilation in children with quadrifoliate valves in the absence of significant valvar dysfunction. We wonder whether significant regurgitation may develop, or become worse, due to progressive dilation of the root as seen in patients with bifoliate valves. It is likely that this possibility will only be resolved by analysis of a larger group of children with congenitally quadricuspid valves.
Acknowledgements
We thank Marzia Petralia for her help and her patience in preparing the figures.







