A 33-year-old man was admitted with chest pain lasting for one year. This lasted for from 3 to 5 minutes and radiated to his back, but was not related to effort. His only risk factor for coronary arterial disease was smoking. No abnormalities were found on physical examination. The electrocardiogram showed depression of 0.5 millimetres in the ST segment, and inversion of the T-wave in leads III and aVF. On transthoracic echocardiography, modified parasternal short axis views (Fig. 1) revealed a contractile diverticulum of 2.7 by 1.5 centimetres projecting from the inferior wall of the left ventricle at its junction with the ventricular septum. Flow could be demonstrated from the diverticulum to the left ventricle using pulsed wave Doppler. Following a positive exercise test, coronary angiography was performed and was normal. On the left ventriculogram in the right anterior oblique projection (Fig. 2), the presence of the contractile diverticulum was confirmed in the mid region of the inferior wall. A decision was made to manage the patient medically with only low dose aspirin, at 100 milligrams per day, and he was discharged with arrangements for follow-up.

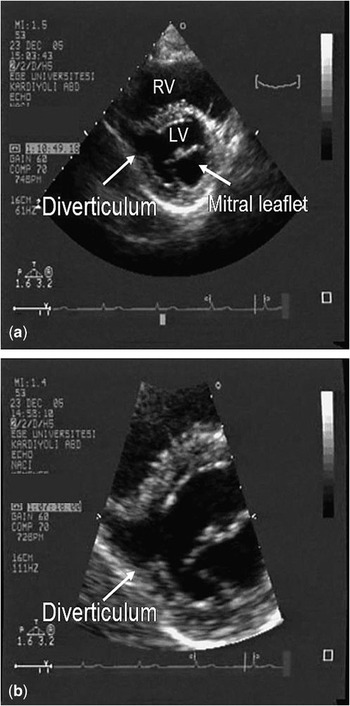
Figure 1 Left ventricular diverticulum (arrow) shown in a normal (a) and close (b) modified parasternal short axis views on the transthoracic echocardiography. RV: right ventricle; LV: left ventricle.

Figure 2 Left ventriculography shows the diverticulum in the right anterior oblique position of the inferior wall.
Congenital left ventricular diverticulum is a rare cardiac anomaly, which forms as a result of protrusion of the endocardium and the myocardium from the free wall of the left ventricle. It is generally an incidental diagnosis in an asymptomatic patient. Rarely, however, the diverticulum can cause chest pain and electrocardiographic changes suggestive of angina pectoris,Reference Ho, Sim, Lee and Chia1 as seen in our case, or lead to the more serious complications of systemic embolism, ventricular arrhythmia, cardiac rupture, heart failure and sudden cardiac death. A congenital left ventricular diverticulum, therefore, should be considered in the differential diagnosis of a young patient with chest pain, and can be confirmed using transthoracic echocardiography.