Congenital supravalvular aortic stenosis is a rare pathology that is defined as severe narrowing of the sinotubular junction of the aorta. A genetic disorder of elastin protein expression is responsible for this defect, which can be either sporadic or inherited. An association between Williams–Beuren syndrome, which is mostly characterised by mental retardation and dysmorphic facial features, and supravalvular aortic stenosis has also been noted. Reference Fricke, d’Udekem and Brizard1–Reference Mongé, Eltayeb and Costello3
Various surgical techniques have been described to treat this congenital anomaly; however, the optimal surgical approach is still controversial. Reference Mitchell and Goldberg4 Surgical augmentation of the stenotic segment from the ascending aorta to the non-coronary sinus with a single patch was described by McGoon et al. Reference Padalino, Frigo and Comisso5 Subsequently, Doty et al Reference Imamura, Prodhan and Dossey6 introduced a technique to relieve the stenosis by augmenting the non-coronary and the right sinuses with a pantaloon-shaped patch. Recently, three-sinus enlargement methods such as three-patch and sliding aortoplasty were advocated to be a better alternative in the present cohorts. Reference Fricke, d’Udekem and Brizard1,Reference Mongé, Eltayeb and Costello3,Reference Imamura, Prodhan and Dossey6 In this report, we aimed to compare the outcomes of the McGoon and the Doty techniques as performed in our clinic.
Materials and methods
This retrospective study was approved by University of Health Sciences Dr. Siyami Ersek Cardiovascular and Thoracic Surgery Training and Research Hospital institutional ethics committee (IRB:280011928-604.01.01). The patients’ demographics, operational, and post-operative follow-up data were obtained from the hospital records. The primary outcome of interest was to compare the re-operation rates of the patients who underwent the McGoon procedure and those who underwent the Doty procedure. The secondary outcome was the potential post-operative results for each group. Each patient’s pre-operative and post-operative cardiac anatomy was evaluated with echocardiography. If the echocardiography results were not clear, angiographic evaluation was performed. Echocardiographic evaluation was completed for all patients pre-operatively, before discharge and post-operatively between 6 months and 1 year. Post-operative echocardiographic findings, re-operations for recurrence, morbidity and mortality were evaluated as follow-up data. The residual gradient of the operated supravalvular aortic stenosis was defined as peak pressure value greater than 40 mmHg. In-hospital mortality was defined as mortality occurring before discharge from hospital. The long-term mortality data were obtained from the National Healthcare Registry.
Patients
Between May 2004 and January 2020, 29 patients underwent repair of supravalvular aortic stenosis in our clinic. Both the McGoon single-patch technique and the Doty technique were used in our department until 2017, and since then only the Doty technique has been used.
Patients whose primary diagnosis was supravalvular aortic stenosis were included in our cohort. Re-operations of this pathology and left ventricular outflow tract obstructions were excluded. Fifteen patients were treated with the Doty technique, and 14 patients underwent the McGoon procedure. Concomitant cardiac lesions were treated at the time of the initial operation. The most common associated lesion was pulmonary stenosis.
Surgical technique
Standard aortic and bi-caval cardiopulmonary bypass settings were initiated for this procedure. Cardiac arrest was accomplished via blood cardioplegia, moderate hypothermia, and cross-clamping. The segment where the stenosis was located was incised longitudinally from the ascending aorta to the non-coronary aortic sinus (Figs 1 and 2). The stenotic segment was enlarged with a diamond-shaped patch in the McGoon technique (Fig 3). In the Doty technique, the incision was made as an inverted Y-shape from the ascending aorta through the non-coronary and the right coronary sinuses, leaving the right coronary ostium on the medial (Fig 4). A pantaloon-shaped patch was placed in the enlarged section of the aorta (Fig 5). The patients were weaned from bypass after the reconstruction of the aorta in the usual fashion. Prior to removal of the cannulas, adequate relief of the supravalvular region of the aorta was confirmed via direct pressure measurements. Associated lesions were repaired during the cross-clamp time.

Figure 1. Pre-operative appearance of supravalvular aortic stenosis.

Figure 2. McGoon incision from ascending aorta to non-coronary aortic sinus.

Figure 3. McGoon patch augmentation of supravalvular aortic segment.

Figure 4. Reverse “Y”-shaped Doty incision from ascending aorta to non-coronary and right coronary aortic sinuses.

Figure 5. Doty patch augmentation of supravalvular aortic segment.
Glutaraldehyde-treated autologous pericardium was mostly used as the patch material; however, synthetic materials such as Dacron®, Gore-Tex®, and other PTFE patches were also used. Extracorporeal membrane oxygenation was used due to deterioration of haemodynamic status in one patient.
Statistical analysis
SPSS (IBM Inc., Armonk, NY, USA) software was used for the statistical analysis. Continuous data are presented as medians with interquartile ranges. Categorical data are reported as frequencies and percentages. The comparison of the continuous data between the groups was analysed with the Mann−Whitney U-test, and the Pearson chi-square test and Fisher’s exact test were used for analysing the categorical data. The Kaplan–Meier method was used for freedom from re-operation with a 95% confidence interval. The log-rank test was used to compare freedom from re-operation between the groups. A p-value > 0.05 is considered statistically significant.
Results
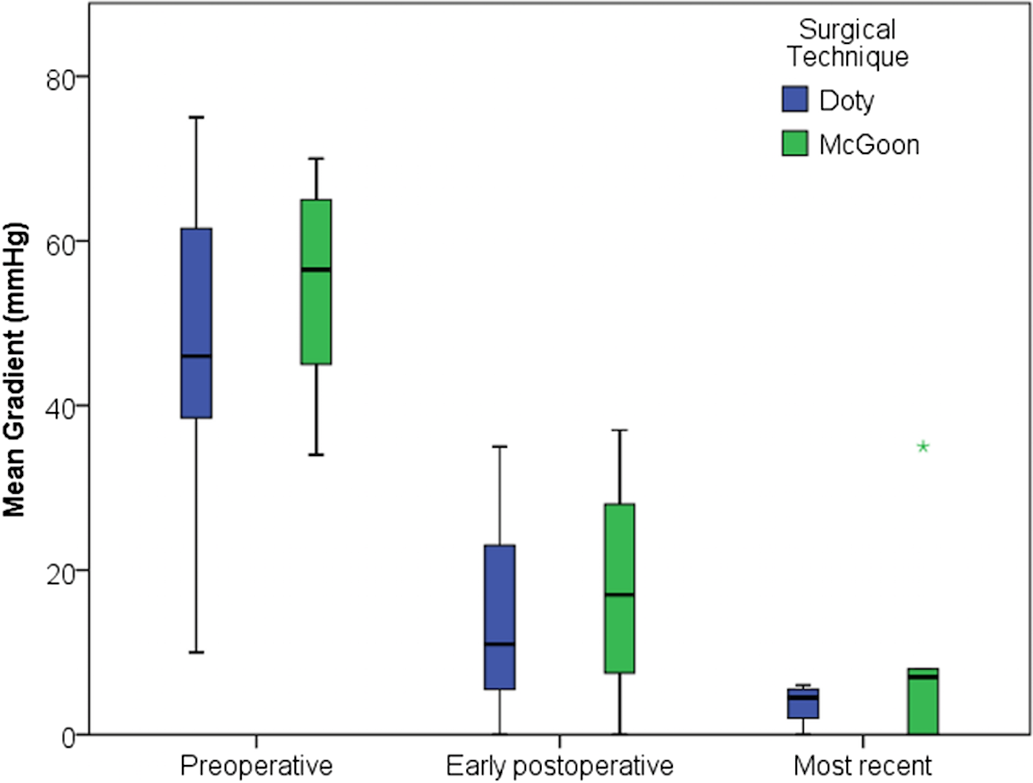
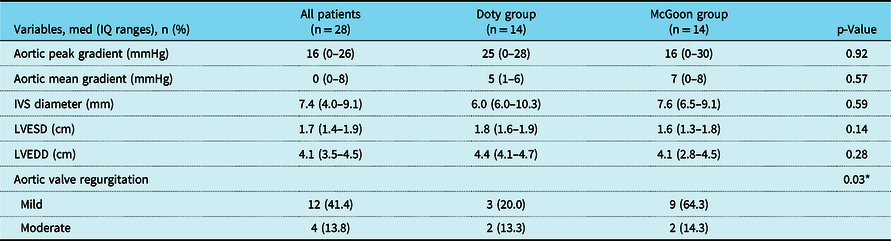
The pre-operative patient data are presented in Table 1. There was no significant difference between the patient groups in demographic data and the pre-operative echocardiographic findings, except that the difference between groups considering the structure of the stenosis was statistically significant (p = 0.01). One patient had Noonan syndrome and 10 patients had Williams–Beuren syndrome. According to the operative findings, there was no significant difference between the groups (Table 2). During the post-operative course, no adverse events were recorded in our cohort. Before discharge, five patients in the McGoon group had a residual supravalvular gradient and one patient in the Doty group (p = 0.05). The mean and peak gradient changes over time for both groups are shown in Figures 6 and 7.

Figure 6. Perioperative mean gradient plot for Doty and McGoon groups.

Figure 7. Perioperative peak gradient plot for Doty and McGoon groups.
Table 1. Pre-operative demographic findings

AS = aortic stenosis; IVS = interventricular septum; LVEDD = left ventricular end-diastolic diameter; LVESD = left ventricular end-systolic diameter; PS = pulmonary stenosis.
* Statistically significant parameter.
Table 2. Operative variables
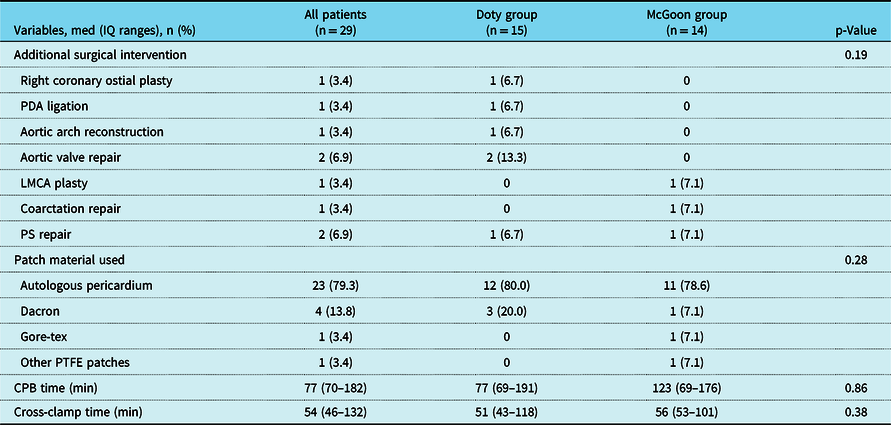
CPB = cardiopulmonary bypass; LMCA = left main coronary artery; PDA = patent ductus arteriosus; PS = pulmonary stenosis; PTFE = polytetrafluoroethylene.
*Statistically significant parameter.
The in-hospital post-operative findings are summarised in Table 3. Follow-up was completed for 92% of the patients, and the median follow-up time was 2.5 (0.7–7.3) years. The longest follow-up time was 16 years. The echocardiographic findings from follow-up are summarised in Table 4.
Table 3. Post-operative findings of the patients

IVS = interventricular septum; LVEDD = left ventricular end-diastolic diameter; LVESD = left ventricular end-systolic diameter; ECMO = Extracorporeal membrane oxigenator; LOS = Lenght of stay
* Statistically significant parameter.
Table 4. Echocardiographic findings of the patients in follow-up

IVS = interventricular septum; LVEDD = left ventricular end-diastolic diameter; LVESD = left ventricular end-systolic diameter.
* Statistically significant parameter.
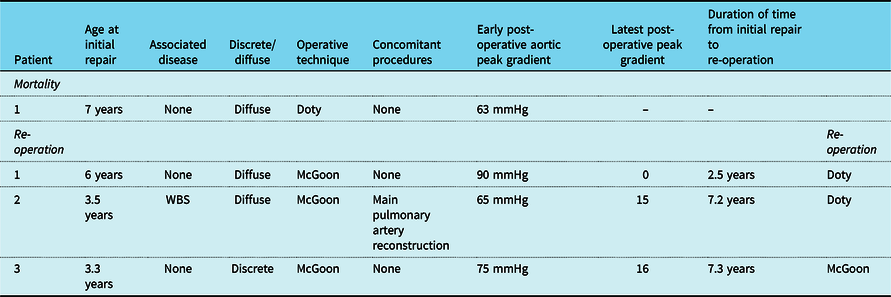
There was no operative mortality in our cohort; however, one patient died post-operatively in the Doty group. The patient was a 7-year-old boy with severe and diffuse supravalvular aortic stenosis. Malign arrhythmia occurred in the post-operative course, and extracorporeal membrane oxygenation was initiated in the ICU. He died due to bleeding complications on the seventh post-operative day.
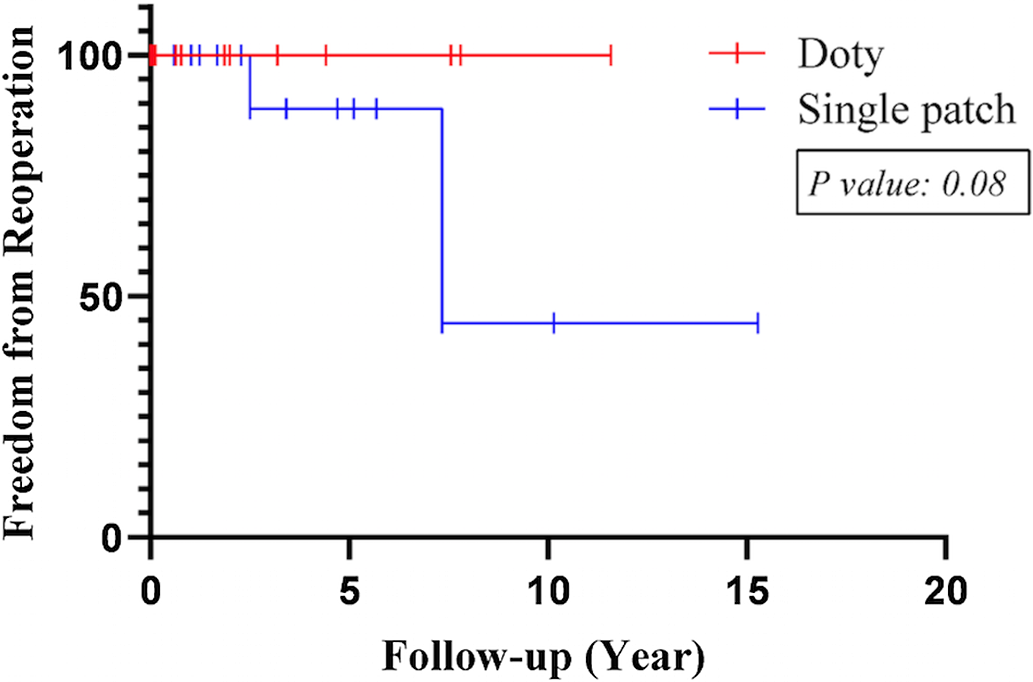
In the long-term period, there was no mortality in our cohort. Three patients in the McGoon group needed re-operation due to residual stenosis, while no patients in the Doty group required re-operation (p = 0.05). The Doty technique was performed as a re-operation for two patients by resecting the Mcgoon patch and replacing a pantaloon-shaped patch. In addition, the Mcgoon technique was re-performed with a larger patch for one patient. Comparing the rates of freedom from re-operation, the 1-, 3-, 5-, and 10-year freedom from re-operation rates in the Doty group were 100%, while the 1-, 3-, and 7-year rates in the McGoon group were 100, 88.9, and 44.4%, respectively (Fig 8). There was no significant difference between the groups in terms of freedom from re-operation rates (p = 0.08). All the re-operated patients had recurrent stenosis of the supravalvular area with a peak gradient of 60 mmHg and above and were treated with glutaraldehyde-treated pericardium. The patient characteristics in relation to mortality and re-operations are summarised in Table 5. Additional problems were not observed in the re-operated patients in the post-operative follow-up period.

Figure 8. Kaplan–Meier analysis of freedom from re-operation for Doty and McGoon group.
Table 5. Patient characteristics of mortality and re-operations

Discussion
Supravalvular aortic stenosis is a progressive arteriopathy, which is commonly associated with Williams–Beuren syndrome Reference Fricke, d’Udekem and Brizard1–Reference Mongé, Eltayeb and Costello3 and affects the great arteries and mostly the supravalvular segment of the aorta, The pathological appearance of the stenotic aortic wall can be discrete or diffuse at the sinotubular junction level, which indicates the degree of the elastin gene defect. The diffuse type of stenosis and Williams–Beuren syndrome lie at the severe side of the spectrum with associated multifocal vascular lesions. Reference Mitchell and Goldberg4 Thus, the diffuse type of aortic pathology has been found to be a risk factor for re-operation Reference Mitchell and Goldberg4–Reference Liu, Gao and Sun7 and reported as a risk factor for mortality. Reference Deo, Burkhart and Dearani8,Reference Deo, Burkhart and Schaff9 In our cohort, two out of three of the patients who were re-operated on and the one patient who died had a diffuse structure. Hence, one of the factors that caused death and reintervention in our cohort could be diffuse structural type.
Pulmonary arterial stenosis is stated to be a risk factor for re-operation, which reflects the severity of the disease. Reference Padalino, Frigo and Comisso5,Reference Imamura, Prodhan and Dossey6 Pulmonary stenosis accompanied by supravalvular aortic stenosis leads to biventricular pressure overload and cardiac complications of stenotic outflow valves. Reference Mitchell and Goldberg4 The intervention rate for concomitant pulmonary stenosis at initial repair has been reported as 41 over 125 patients(32%) in a multi-center study, Reference Padalino, Frigo and Comisso5 which compares with approximately 16% of the patients in our cohort with pulmonary stenosis at the initial repair who had an intervention. In addition, only one re-operated patient had concomitant pulmonary stenosis at the initial procedure. We can attribute this difference to a lower incidence of Williams–Beuren syndrome in our cohort.
Diffuse structural disease of the aorta and the branch pulmonary arteries are the main characteristics of the cardiovascular anomalies of Williams–Beuren syndrome. Despite the severe nature of this disease, surgical treatment with excellent outcomes can be achieved. Reference Fricke, d’Udekem and Brizard1,Reference Cha, Song and Lee2 One-third of our cohort had Williams–Beuren syndrome; however, only one patient who was re-operated on had this syndrome. Aggressive progression of the disease results in the early onset of clinical symptoms and reflects the severity of the pathology. However, this syndrome has not been defined as a risk factor for adverse cardiac events. Conversely, the diffuse structural pathology and pulmonary lesions that are also associated with Williams–Beuren syndrome have been stated as risk factors. Reference Padalino, Frigo and Comisso5,Reference Deo, Burkhart and Schaff9
Surgical treatment with different techniques has been advocated with remarkable outcomes. Reference Fricke, d’Udekem and Brizard1,Reference Mongé, Eltayeb and Costello3,Reference Padalino, Frigo and Comisso5,Reference Liu, Gao and Sun7,Reference Wu, Mondal and del Nido10 There are several methods described other than the McGoon and Doty procedures, such as the Brom three-patch technique, the Myers interdigitating technique, and a two separate patches technique; however, there is no consensus about a superior technique. Reference Deo, Burkhart and Dearani8,Reference Bakhtiary, Amer and Etz11,Reference Roemers, Kluin and de Heer12 According to a multi-center study, the single- and pantaloon-patch methods were the most preferred two surgical techniques among surgeons with both 110 patients (36.7%); however, no superiority was noted. Reference Padalino, Frigo and Comisso5 Both techniques have been found to be simple, reproducible and have excellent outcomes, and the authors pointed out that patient-specific procedures provide better results in their experience. Reference Deo, Burkhart and Dearani8 Conversely, other reports have indicated that the Doty procedure was superior to the single-patch technique in relation to freedom from re-operation. Reference Ibarra, Spigel and John13,Reference Kaushal, Backer and Patel14 Regarding our data, we can speculate that the Doty procedure was superior, considering the re-operation rates. However, the freedom from re-operation estimates showed no significant difference. This result can be attributed to the good outcomes of the McGoon single-patch repair until the fifth year of follow-up. Ibarra et al stated that estimates of freedom from re-operation were 67% at the 10th year after the initial operation, which compared to 44.4% in our cohort.
Surgical treatment of supravalvular aortic stenosis has been performed with good survival outcomes, Reference Padalino, Frigo and Comisso5,Reference Imamura, Prodhan and Dossey6,Reference Deo, Burkhart and Schaff9,Reference Wu, Mondal and del Nido10,Reference Roemers, Kluin and de Heer12 and no significant difference between operational techniques has been found in terms of survival. Reference Roemers, Kluin and de Heer12,Reference Kramer, Absi and Hetzer15 The single early death in our cohort had the Doty procedure; however, this result cannot only be attributed to the surgical method considering the patient’s risk factors. Early infancy at initial repair, a higher residual gradient, pre-existing aortic stenosis, and diffuse type lesions have been reported to be risk factors for survival. Reference Padalino, Frigo and Comisso5,Reference Deo, Burkhart and Dearani8 Roemers et al Reference Roemers, Kluin and de Heer12 reported in their 52-year experience that in the long-term follow-up, survival of the operated patients was remarkably low compared with the general population, and thus close follow-up is recommended.
Coronary artery ostial narrowing is one of the aetiologic factors that associated with myocardial ischaemia which can lead to probable early and late mortality for supravalvular aortic stenosis. Reference Padalino, Frigo and Comisso5 The incidence of this concomitant anomaly ranges between 1 and 26% of cohorts. Reference Imamura, Prodhan and Dossey6,Reference Deo, Burkhart and Dearani8–Reference Wu, Mondal and del Nido10 It was reported that concomitant surgical intervention of coronaries were required for 26% of patients with ostial coronary stenosis in a series Reference Wu, Mondal and del Nido10 ; contrarily, there are reports that none of the patients had concomitant coronary intervention in their cohorts. Reference Liu, Gao and Sun7,Reference Deo, Burkhart and Schaff9 Most of the lesions were treated with resection of excessive tissues around the ostium of coronaries. Reference Wu, Mondal and del Nido10 Conversely, patch augmentation of the coronaries can be performed for other ostial anomalies. Reference Padalino, Frigo and Comisso5,Reference Deo, Burkhart and Dearani8 In our cohort, there were two patients underwent a concomitant coronary intervention. One patient with right coronary ostial stenosis had patch augmentation by extending one leg of the patch to coronary with the Doty technique and the other patient was in McGoon group and had patch augmentation of left main coronary stenosis with a different separate patch. It was advocated that three-patch repair had a better relief on coronary arteries considering the ease of placement of the patches. Reference Mongé, Eltayeb and Costello3
The single-patch and the Doty techniques are commonly performed, but there has been a tendency to change the operational strategy to symmetrical reconstructions such as the Brom method, despite longer cross-clamp times and related problems. Reference Fricke, d’Udekem and Brizard1,Reference Mongé, Eltayeb and Costello3,Reference Imamura, Prodhan and Dossey6,Reference Kaushal, Backer and Patel14,Reference Kramer, Absi and Hetzer15 Although there are no data on the long-term outcomes of these symmetrical reconstruction methods, recent studies have indicated promising results. Reference Fricke, d’Udekem and Brizard1,Reference Kramer, Absi and Hetzer15 Considering the disadvantages of those procedures, we have no intention to change our strategy to symmetric repair. Symmetrical aortic sinus repairs have been found to result in a lower post-operative gradient, which is associated with lower re-operation rates. Reference Mongé, Eltayeb and Costello3,Reference Kaushal, Backer and Patel14 However, three-sinus repair techniques have not been found to be statistically superior in terms of time-related analysis. Reference Kramer, Absi and Hetzer15 A post-procedural aortic residual gradient has been stated as a predictor of mortality. Reference Deo, Burkhart and Dearani8,Reference Deo, Burkhart and Schaff9 Although a residual gradient was not defined as a risk factor for re-operation in recent studies, in our cohort all the patients who underwent re-operation had a post-operative peak gradient above 40 mmHg. Kaushal et al Reference Kaushal, Backer and Patel14 stated that their choice of technique evolved from the single-patch to the Brom method due to higher residual pressure gradients and a higher rate of re-operations. Likewise, a similar transformation occurred gradually from the McGoon to the Doty technique in our clinic.
Limitations
The main limitation of this study was its retrospective data collection. Our clinic is a referral centre for paediatric cardiovascular cases and accepts patients from all around the country; thus, patient follow-up data retrieval can be problematic. The rarity of the disease and therefore the small number of patients and shorter follow-up times also limit speculation on firm conclusions from this study. Risk analysis could not be performed due to the small numbers of deaths and re-operations.
Conclusion
Supravalvular aortic stenosis can be treated with different surgical techniques with good outcomes. Compared to patients who were operated on with the McGoon technique, the number of patients who had a post-operative residual supravalvular gradient was lower in the patients who were operated on with the Doty method. Hence, considering the re-operation rates after initial reconstruction surgery, we can speculate that the Doty technique was superior.
Acknowledgements
M.B.: writer, literature review, data collection, conception and design; M.D.: data collection and statistical analysis; O.K.: critical review and statistical analysis; H.F.A.: data collection and critical review; O.Y.: data collection; M.Ç.: data collection; F.Ö.: data collection; A.S.: data collection; Y.A.: data collection and supervision; I.K.Y.: data collection and supervision; A.Ş.: approval and supervision; and N.A.A.: approval and supervision; The authors wanted to thank Ahmet Elibol M.D.(elibol.md@gmail.com) for the medical illustrations.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of interest
None.