


Hearts in which the aortas arise from the morphologically left ventricle, but with an unexpected relationship of their roots to the pulmonary trunks, have long fascinated cardiac anatomists and paediatric cardiologists. In such settings, the concordant nature of the ventriculo-arterial connections means that the abnormal arrangement, in itself, does not disturb the haemodynamic pathways through the heart. The unexpected relationships of the arterial roots, however, can produce problems in diagnosis. Over the years, the hearts have produced even greater problems for those seeking to find the optimal means of description. The presence of an aortic root positioned anteriorly relative to the pulmonary trunk, with the leaflets of the aortic valve supported by a completely muscular infundibulum, was initially the accepted criterion for the definition of “transposition”. Therefore, in the reported cases, because the anterior aorta had retained its origin from the morphologically left ventricle, the presumed transposition was said to be “anatomically corrected”.Reference Harris and Farber 1 Some distinguished authorities, however, queried the existence of such hearts, suggesting that they represented an embryological impossibility.Reference Van Mierop and Wiglesworth 2 Increasing experience, nonetheless, coupled with progress in diagnostic techniques, showed that the ventriculo-arterial connections could be concordant, despite the abnormal position of the aortic root.Reference Van Praagh and Van Praagh 3 It was subsequent to further discussions relating to the definition of “transposition” itselfReference Van Mierop 4 , Reference Van Praagh 5 that the arrangement with the anteriorly located aorta arising from the left ventricle, and with its valve supported by a completely muscular infundibulum, became re-named as “anatomically corrected malposition”.Reference Kirklin, Pacifico, Bargeron and Soto 6 It was then shown that the unexpected patterns at the ventriculo-arterial junctions could be found with various arrangements across the atrioventricular junctions, including discordant ones.Reference Anderson, Becker, Losekoot and Gerlis 7 The combination of concordant ventriculo-arterial with discordant atrioventricular connections was particularly important, as it produced the haemodynamic pattern of “transposition”, despite the fact that the arterial trunks arose from their appropriate ventricles.Reference Kirklin, Pacifico, Bargeron and Soto 6 , Reference Anderson, Becker, Losekoot and Gerlis 7 This, of course, is because discordance is found only at the level of the atrioventricular junctions, unlike congenitally corrected transposition, where there is double discordance. Owing to the discordance at only one of the junctions, the combination also provides the ideal situation for surgical repair using atrial re-direction, rather than the arterial switch, as the aorta remains supported by the morphologically left ventricle.Reference Arciprete, Macartey, de Leva and Stark 8
From the stance of description, for those using the concept of segmental diagnosis, the entity known as “anatomically corrected malposition” was also required to have the aortic valve, arising from the morphologically left ventricle, supported by a completely muscular infundibum.Reference Van Praagh and Van Praagh 3 Those using this approach had also observed that, when such an infundibulum was lacking in patients with usual atrial arrangement, concordant ventriculo-arterial but with discordant atrioventricular connections such that the aortic valvar leaflets were in fibrous continuity with the leaflets of the mitral valve, the aortic root was usually positioned posteriorly and rightward relative to the pulmonary root.Reference Van Praagh and Van Praagh 9 These, of course, are the relationships of the arterial roots found in the normal heart. Therefore, because of this apparently normal relationship of the arterial roots, coupled with the usual arrangement of the atrial chambers, the proponents of the segmental approach argued that the combination represented “isolated ventricular inversion” rather than “anatomically corrected transposition”.Reference Van Praagh and Van Praagh 9 They also presumed that, in other patients with discordant atrioventricular connections, the arterial trunks could arise from the ventricular mass in their anticipated spiralling manner. They then argued that, if the atrial chambers were mirror-imaged with this combination, the entity would represent “isolated atrial inversion”, as the ventricular mass and the arterial trunks would be found in their expected positions.Reference Van Praagh 10 To the best of our knowledge, however, hearts with mirror-imaged atrial appendages, discordant atrioventricular connections, and concordant ventriculo-arterial connections with spiralling arterial trunks have yet to be described. The hearts we have encountered that match most closely with this combination have had left-handed ventricular topology in the setting of isomeric, rather than mirror-imaged, atrial appendages. The presence of the isomeric atrial appendages means that, rather than being discordant, the atrioventricular connections show mixed morphology, with half of the atrioventricular junctions being concordantly connected, but the other half connected in a discordant manner. We had previously termed this an ambiguous arrangement.Reference Anderson and Ho 11 We now consider it best described in terms of mixed atrioventricular connections.Reference Anderson and Shirali 12 In some hearts having isomeric atrial appendages, nonetheless, the venoatrial connections can be such as to produce either quasi-normal or quasi-mirror-imaged haemodynamic patterns of flow.Reference Macartney, Zuberbuhler and Anderson 13 If such quasi-normal venoatrial connections were present in patients with left isomerism and left-handed ventricular topology, the pathways of flow through such hearts would be virtually identical to those with truly discordant atrioventricular connections. In contrast, the combination of quasi-mirror-imaged venoatrial connections, isomeric atrial appendages with mixed atrioventricular connections, and left-handed ventricular topology with concordant ventriculo-arterial connections and spiralling arterial trunks would be equivalent to the arrangement described as “isolated atrial inversion” by those using the segmental approach.Reference Van Praagh 10 It is, of course, the haemodynamic pathways that determine the optimal therapeutic pathways. The question remains, therefore, as how best to describe these unusual hearts, optimising the chances not only for correct diagnosis but also for the choice of the appropriate surgical therapies. It is our opinion that the best solution is provided by the use of sequential segmental analysis,Reference Cavalle-Garrido, Bernasconi, Perrin and Anderson 14 using the concept of the “morphological method”Reference Van Praagh, David, Wright and Van Praagh 15 to determine the precise arrangement of the atrial chambers. Our previous experience, nonetheless, has identified potential problems in determining ventricular topology. In addition, therefore, we address this issue, as recognition of the topological arrangement of the ventricular mass is another key factor to understanding these complex cardiac malformations.
The normal ventriculo-arterial junctions
In a normally constructed heart, the pulmonary trunk arises from the morphologically right ventricle, supported by the free-standing muscular infundibular sleeve. It then spirals around the right-sided aortic root as it extends posteriorly before bifurcating into the right and left pulmonary arteries at the margins of the pericardial cavity (Fig 1a). The pulmonary trunk, therefore, exits from the pericardial cavity on the opposite side of the aorta relative to the systemic venous atrium. The leaflets of the aortic valve, which is right-sided relative to the pulmonary root in the normal heart, are in fibrous continuity with the leaflets of the left-sided mitral valve (Fig 1b). In this normal arrangement, the right ventricle shows right-handed topology, and the pulmonary trunk passes to the left of the aortic root as it exits from the pericardial cavity (Fig 1a).

Figure 1 The images taken from a normal heart show the features of the ventriculo-arterial junctions. ( a ) The windowed right atrium and ventricle viewed from the right anterior oblique aspect. The arterial trunks spiral as they leave the base of the ventricular mass, with the free-standing infundibular muscular sleeve lifting the leaflets of the pulmonary valve away from the cardiac base. As the pulmonary trunk exits from the pericardial cavity, it passes to the left of the ascending aorta. ( b ) The inferior aspect of the aortic root as viewed from the cardiac apex. The leaflets of the normally positioned right-sided aortic valve are in fibrous continuity with the left-sided mitral valve (double-headed red arrow).
In the setting of the mirror-imaged normal heart, as seen sometimes in so-called “situs inversus”, these relationships are themselves mirror-imaged. Thus, the arterial trunks spiral as they extend from the cardiac base to the mediastinum, but the aortic root is posterior and left-sided relative to the pulmonary trunk (Fig 2a). Moreover, as it exits from the left-sided morphologically right ventricle, the infundibulum extends from left to right (Fig 2b). The leaflets of the right-sided mitral valve are then in fibrous continuity with those of the left-sided aortic valve in the roof of the right-sided morphologically left ventricle.

Figure 2 The images show the features of a normal heart from an individual with mirror-imaged arrangement of the bodily organs; ( a ) shows how, in the setting of mirror-imagery, the pulmonary trunk spirals from left to right around the left-sided aortic root, which arises from the right-sided morphologically left ventricle. ( b ) The internal architecture of the left-sided morphologically right ventricle. There is left-handed ventricular topology, with the infundibulum extending rightward as it supports the leaflets of the pulmonary valve.
The concept of ventricular topology
The essence of topology is that the morphology of structures with a given topological arrangement cannot be altered simply by the process of rotation or tilting. Their topological make-up can only be changed by the physical act of dismembering their component parts, and then re-assembling them in an altered manner. On this basis, the parietal structures within the body can be recognised as representing topological isomers in the same individual. The exemplars of bodily isomerism, therefore, are the hands. The arrangements of all the parietal right-sided and left-sided body components could equally well be taken as representing bodily isomerism. It is the isomeric arrangement of the hands, nonetheless, which we consider to illustrate the topological arrangement of the ventricular mass, with the morphologically right ventricle being used as a representative for this purpose. Thus, when assessing the normal right ventricle, it is only the right hand that can be placed on the ventricular septal surface such that the thumb is on the inlet, the palm is on the apical muscular septum, and the fingers extend into the subpulmonary infundibulum (Fig 3a). This normal arrangement of the ventricular mass, therefore, can be described as showing right-handed topology. This is the equivalent of right-handed ventricular looping, listed as “D” in segmental notation.Reference Van Praagh 10 Left-handed ventricular topology has already been illustrated in Figure 2b, which showed the mirror-imaged ventricular mass in a patient with mirror-imaged atrial chambers and concordant atrioventricular connections. Left-handed topology is also represented by the morphologically right ventricle in patients having congenitally corrected transposition in the setting of usual atrial arrangement (Fig 3b). Such left-handed ventricular topology is equivalent to left-handed ventricular looping, and is listed as “L” in segmental notation.Reference Van Praagh 10

Figure 3 The images show how the hands can be used to determine the topological arrangement of the ventricular mass, taking the morphologically right ventricle as being representative of the overall arrangement. In the normal heart ( a ), it is only the right hand that can be placed on the ventricular septal surface such that the thumb fits the tricuspid valve and the fingers lie on the infundibulum. In the typical arrangement of congenitally corrected transposition with usual atrial arrangement, in contrast, it is the left hand that can be placed in a comparable way on the septal surface of the morphologically right ventricle. Such left-handed topology is also seen in ( b ), which shows the mirror-imaged right ventricle in an individual with mirror-imaged atrial chambers and concordant atrioventricular connections. As with the hands themselves, the topological arrangement of the ventricular mass cannot be altered simply by rotation or tilting. In each instance, it is also the case that the left hand could be placed on the septal surface of the morphologically left ventricle, but it is the right ventricle that is arbitrarily used to determine the topological arrangementReference Anderson and Ho 11 or the direction of ventricular looping by those who use segmental notation.Reference Van Praagh 10
The morphological method
This concept, based on a principle first suggested by Lev,Reference Lev 16 was formulated by Van Praagh et alReference Macartney, Zuberbuhler and Anderson 13 while criticising a paper written in part by one of the current authors.Reference Uemura, Ho, Devine, Kilpatrick and Anderson 17 The topic under discussion had been the nature of the small ventricular chamber found in the setting of double-inlet right ventricle. The authors of the original article had suggested that this small chamber could be disqualified from left ventricular status because it lacked its inlet portion.Reference Uemura, Ho, Devine, Kilpatrick and Anderson 17 Van Praagh et alReference Macartney, Zuberbuhler and Anderson 13 identified a fundamental flaw in this proposed logic. They argued, correctly, that it was inappropriate to name one structure, which was itself variable – in this instance the morphologically left ventricle – on the basis of another structure, which was also variable – namely, the ventricular inlet. The essence of the morphological method, therefore, was that structures within the heart should be defined and named on the basis of their own intrinsic anatomy. This method is exemplified by considering hearts from patients with totally anomalous pulmonary venous connection (Fig 4). As shown, if the connections of the pulmonary veins were used as the criterion for identification of the left atrium in the setting of totally anomalous pulmonary venous connection, then it is the liver that would be identified as the left atrium when there is infra-diaphragmatic drainage. The morphological method dictates that, instead, the most constant atrial component should be used for the purposes of definition. As shown in Figure 4, this is readily achieved when using the appendage for this purpose. This principle proves to be of particular value when assessing hearts from patients with so-called “visceral heterotaxy”. This is because, in this setting, it is well established that the veno-atrial connections are particularly variable. Sometimes, nonetheless, they can be arranged to produce quasi-normal or quasi-mirror-imaged patterns of venous return.Reference Macartney, Zuberbuhler and Anderson 13 Even in this setting, however, when using the extent of the pectinate muscles relative to the atrioventricular junctions to distinguish morphological rightness from leftness (Fig 5), it is possible to distinguish the hearts as having either isomeric right or isomeric left atrial appendages.Reference Uemura, Ho, Devine, Kilpatrick and Anderson 17

Figure 4 The image shows a heart from a patient with totally anomalous pulmonary venous connection to a vertical vein that passes through the diaphragm and drains to the hepatic portal venous system. If, in this situation, the connection of the pulmonary vein had been used to identify the left atrium, as suggested by those using the segmental approach to diagnosis,Reference Van Praagh 10 then the liver would, automatically, be identified as the left atrium. As can be seen, the presence of the left atrial appendage, the most constant component of the atrial chambers, permits the morphologically left atrium to be identified in its own right. This is the logic that underscores the principle of the morphological method.Reference Macartney, Zuberbuhler and Anderson 13

Figure 5 The image has been constructed by taking a heart with hypoplasia of the morphologically left ventricle and sectioning it in a “four-chamber” fashion. The caudal part of the heart is imaged from the front in the left-hand half of the picture, whereas the cranial part is shown from the back to the right hand. The extent of the pectinate muscles relative to the atrioventricular junctions clearly distinguishes between the morphologically right and left atrial appendages. The pectinate muscles extend to the crux in the right atrium, but are confined within the tubular appendage in the left atrium.
In this regard, we should stress that, within the heart, it is only the appendages that are truly isomeric. The other cardiac features and the veno-atrial connections, in particular, require full description. It is the veno-atrial connections together with the connections across the atrioventricular and ventriculo-arterial junctions that determine the patterns of flow through the heart. In addition, as we have already emphasised, these are the pathways that determine the optimal approach when deciding on surgical correction. It is also well established, nonetheless, that there is an excellent correlation between bronchial morphology and the arrangement of the atrial appendages.Reference Uemura, Ho, Devine, Kilpatrick and Anderson 17 Nevertheless, as we will show, such correlation is not a constant feature, even when both atrial chambers and the bronchial tree are lateralised. Van Mierop et alReference Van Mierop, Eisen and Schiebler 18 showed long since, nonetheless, that the morphology of the bronchial tree could be used to identify the overall arrangement of the bodily organs. Establishment of bronchial morphology, therefore, is of particular value in the setting of so-called “heterotaxy”. It is not unreasonable to suggest that, unless shown otherwise, when there is left bronchial isomerism then the atrial appendages should also be presumed to be isomeric, with the heart analysed as showing left isomerism. As we will also show, this distinction is one of the keys to the appropriate description of the hearts from patients presumed to have “isolated ventricular inversion”, also known as “isolated ventricular discordance”; it is also a key feature in the analysis of so-called “isolated atrial inversion”.Reference Van Praagh 10 Before considering such truly rare combinations, however, we should pay attention to the rare but more frequently encountered lesions, in which the arterial trunks arise from appropriate ventricles but extend into the mediastinum in a parallel as opposed to a spiralling manner, with both their arterial valves supported by completely muscular infundibulums. It was this combination of features that was initially described as “anatomically corrected transposition”,Reference Van Praagh and Van Praagh 3 and is now more usually described as “anatomically corrected malposition”.Reference Van Praagh 10
What is “anatomically corrected malposition”?
The essence of the lesion, when the atrioventricular connections are concordant, is that the flow pathways through the heart are as expected, but the arterial trunks are not arranged in their anticipated manner. Instead of spiralling as they extend from the base of the heart into the mediastinum, such that the pulmonary trunk is positioned on the opposite side of the aorta compared with the location of the morphologically right atrium, the arterial trunks leave the pericardial cavity in a parallel manner, with the pulmonary trunk on the same side as the systemic venous atrium. This combination of features is exemplified by our experience with a 28-year-old woman, who presented recently to the outpatient department of the All India Institute of Medical Sciences in New Delhi for evaluation of a murmur. She had some restrictions in carrying out her activities due to exertional breathlessness, although she had generally been doing well. She also complained of occasional palpitation on exertion. Cardiac examination revealed mild cardiomegaly, with normal heart sounds, and an additional left ventricular third sound heard at auscultation. The pansystolic murmur, graded at 3 out of 6, was heard best at the left upper sternal border. Cross-sectional echocardiography revealed the presence of usual atrial arrangement, along with concordant atrioventricular and ventriculo-arterial connections, although with an unexpected relationship of the arterial roots. Owing to the unexpected echocardiographic findings, we performed computed tomographic angiography. The images confirmed the usual arrangement of the abdominal organs, along with usual atrial arrangement (Fig 6a), with concordant atrioventricular connections and right-handed ventricular topology (Fig 7a).
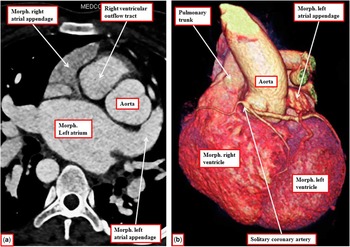
Figure 6 The images are taken from a computed tomographic data set prepared from a patient with usual atrial arrangement, concordant atrioventricular connections (see Fig 7), and concordant ventriculo-arterial connections. The left-hand panel shows the usual arrangement of the atrial appendages, with the right ventricular outflow tract anterior and right-sided relative to the aortic root. The reconstruction shown in the right-hand panel reveals that the intra-pericardial roots are initially parallel to one another as they exit from the base of the heart, although the aorta then swings rightward to continue as a right-sided aortic arch. The pulmonary trunk, however, exits from the pericardial cavity on the same side as the morphologically right atrium.

Figure 7 Panel ( a ) shows a caudal cut through the tomographic data set obtained from the patient shown in Figure 6, illustrating the concordant atrioventricular connections. Panel ( b ) shows the long-axis parasternal echocardiographic cut. The aorta arises from the morphologically (morph.) left ventricle, so that there are concordant ventriculo-arterial connections. Despite being left-sided and posterior, however, the aortic valve is supported by a completely muscular infundibulum.
The aortic root was shown to arise posteriorly and leftward relative to the pulmonary trunk, taking its origin exclusively from the morphologically left ventricle. This is an unusual finding, as the aorta is typically anterior when arising from the left ventricle in the setting of parallel arterial trunks. The pulmonary trunk arose exclusively from the right ventricle, and was supported by an extensive muscular infundibulum. Further analysis of the echocardiographic findings also revealed discontinuity between the leaflets of the aortic and mitral valves, showing that the aorta was arising from the left ventricle above a completely muscular infundibulum (Fig 7b). There was also a ventricular septal defect; three-dimensional reconstruction of the computed tomographic images confirmed that the aortic root was positioned leftward and inferior relative to the subpulmonary infunbibulum. This is the anticipated mirror-imaged variant of “normal relations”; however, in this patient, the aortic valve was supported by a completely muscular infundibulum (Fig 7b). The ascending aorta, furthermore, rather than spiralling from left to right as would be expected for mirror-imaged “normal relations”, extended into the mediastinum parallel to the pulmonary trunk (Fig 6b). The computed tomographic images also revealed the presence of a solitary coronary artery, which arose from the left and anterior aortic sinus, with the right coronary artery extending anteriorly across the subpulmonary infundibulum to reach the right atrioventricular groove (Fig 6b). Despite the unusual arrangement of the arterial trunks, the haemodynamic pathways through the heart were essentially normal. The patient underwent successful surgical closure of the ventricular septal defect, and is doing well.
Problems with the appropriate diagnosis of patients with such rare segmental combinations were illustrated by another patient seen recently at the All India Institute of Medical Sciences in New Delhi. The patient had concordant atrioventricular and ventriculo-arterial connections, but in the setting of mirror-imaged atrial arrangement. When some of us first described this particular patient, we made the diagnosis of “isolated atrial inversion”.Reference Gupta, Gulati, Saxena, Ho and Juneja 19 This was because of problems in determining the ventricular topology in consequence of the marked twisting of the concordant atrioventricular connections (Fig 8). The situation was more complicated, as the patient, with obviously mirror-imaged atrial arrangement, demonstrated the usual branching pattern of the bronchial tree (Fig 9). There was, therefore, discordance between the atrial and bronchial arrangements, although both arrangements were lateralised rather than being isomeric.

Figure 8 The images are from the computed tomographic data set obtained from a patient initially described as having “isolated atrial inversion”.Reference Gupta, Gulati, Saxena, Ho and Juneja 19 As can be seen, the atrial chambers are indeed mirror-images ( a and b ). Panel ( a ), in “Four chamber” projection, however, shows that the left-sided morphologically (morph.) right atrium (RA), with its triangular appendage, is connected in a concordant manner to the morphologically right ventricle (RV), which is anterior and right-sided. The inferior caval vein was also right-sided. As shown in Panel ( b ), however, the atrioventricular connections are twisted, with the right-sided left atrium (LA), with its tubular left appendage, connected to the left-sided and inferior morphologically left ventricle (LV), which gives rise to the aorta. A ventricular septal defect is present directly beneath the aortic root. The red arrows in the panels show the twisted arrangement of the atrioventricular connections, producing the situation also described as the “criss-cross heart”.

Figure 9 Imaging of the bronchial tree from the patient whose heart is illustrated in Figure 8 reveals the presence of usual bronchial arrangement.
The key information with regard to the determination of ventricular topology, nonetheless, is that the atrial chambers, as shown in Figure 8, were mirror-imaged, such that the morphologically right atrium was unequivocally left-sided. The atrioventricular connections, although twisted, were concordant; however, because of the twisting of the ventricular mass, the morphologically right ventricle was anterior and right-sided. The patient underwent cardiac catheterisation, and the course of the catheter used to provide visualisation of the pulmonary trunk showed the inferior caval vein moving from the right to the left side, having crossed the diaphragm to enter the left-sided morphologically right atrium (Fig 10a).

Figure 10 The images show the course of the catheter inserted through the inferior caval vein (ICV) to inject contrast into the pulmonary trunk. The lateral projection ( a ) shows how the catheter enters the morphologically right ventricle through the posteriorly located inlet and then extends anteriorly through the cranially located pulmonary trunk. Panel ( b ) shows the frontal projection. Despite the twisting of the atrioventricular connections and the right-sided location of the apical component of the morphologically right ventricle, we know that the morphologically right atrium is right-sided and posterior. It is the atrial chambers that anchor the heart within the pericardial cavity; because of this anchoring, as shown in panel ( b ), it is only the thumb of the left hand that can be placed on the tricuspid valve, with the fingers on the outlet component, and the palm on the septal surface of the right ventricle. The ventricular mass, therefore, shows left-handed topology despite the presence of twisted atrioventricular connections.
The twisting of the atrioventricular connections and ventricular mass,Reference Seo, Yoo, Ho, Lee and Anderson 20 with the morphologically right ventricle being right-sided, despite the presence of mirror-imaged atrial arrangement and concordant atrioventricular connections (Fig 8), produces the arrangement previously described as the “criss-cross heart”.Reference Anderson, Shinebourne and Gerlis 21 The essence of the malformation is that the ventricular mass is able to rotate on the atrial chambers, which are anchored by the veno-atrial connections within the pericardial cavity. The reconstruction of the computed tomographic data set confirmed the unusual morphology of the ventricular mass. It showed that the concordantly connected pulmonary trunk was on the same side of the aorta as the morphologically right atrium. The patient, therefore, had concordant but twisted atrioventicular connections, concordant ventriculo-arterial connections, and parallel arterial trunks. At the first inspection, the anteriorly located right ventricle seemed to be arranged to show right-handed topology (Fig 11a and b), which would be disharmonious with concordant atrioventricular connections in the setting of mirror-imaged atrial arrangement. This was, indeed, the interpretation of the ventricular morphology when this patient initially presented.Reference Gupta, Gulati, Saxena, Ho and Juneja 19 When we look at Figure 11a, b and c of the reconstructed data set, we can see why the initial diagnosis was of right-handed topology, as Figure 11c is remarkably similar to the arrangement of the normal right ventricle. In the normal situation, however, the tricuspid valve is posterior but right-sided relative to the caudal part of the ventricular septum. In the heart illustrated, because the morphologically right atrium is left-sided, it is only the thumb of the left hand that can be placed on the ventricular inlet, with the palm against the caudal part of the ventricular septum. The larger part of the ventricular septum is, in fact, obliquely orientated. This is the consequence of the counter-clockwise rotation of the ventricular mass, viewed from the apex, relative to the anchored atrial chambers, which are mirror-imaged. This had produced the twisted atrioventricular connections. This can be well seen in Figure 8a. If the arrangement as shown in Figure 11c is, figuratively speaking, untwisted in clockwise direction, again as viewed from the apex, then the septum would be viewed from its left side, as is shown in Figure 11d, with the palm of the left hand then fitting the septal surface. The image that permits the septum to be seen from the left side provides validation of the interpretation based on the catheter course (Fig 10). In terms of segmental connections, therefore, the patient had concordant atrioventricular and ventriculo-arterial connections. The concordantly connected arterial trunks, however, are parallel rather than spiralling as they exit from the ventricular mass, with discontinuity between the leaflets of the aortic and mitral valves (Fig 8b). If described using segmental terminology, therefore, the patient has “anatomically corrected malposition” rather than “isolated atrial inversion”. As was described initially,Reference Gupta, Gulati, Saxena, Ho and Juneja 19 there is marked twisting of the atrioventricular connections, but the atrial and ventricular segments are connected in a harmonious manner, with the anticipated left-handed ventricular topology, despite the right-sided location of the greater part of the morphologically right ventricle.

Figure 11 The computed tomographic images as shown in Figure 8 were reconstructed to provide a three-dimensional view of the overall heart ( a and b ). The pulmonary trunk is on the same side as the mirror-imaged morphologically right atrium, and both are to the left of the aorta. Panel ( c ) is produced by segmenting the data set so as to reconstruct only the right ventricle. At the first sight, there is right-handed topology, but this is only seen relative to the parietal wall of the right ventricle. When the chamber is viewed from the septal aspect ( d ), it can be seen that it is the left hand that fits on the septal surface, with thumb on the inlet, and the fingers in the outflow tract. Despite the marked twisting of the ventricular mass, there is the expected left-handed topology for mirror-imaged atrial chambers and concordant atrioventricular connections.
What, then, is “isolated ventricular discordance”?
Our potential introduction to this very rare lesion happened when we encountered a heart in the archive of the Ann and Robert H. Lurie Children’s Hospital in Chicago. Only the heart was available for examination, and showed the unequivocal features of discordant atrioventricular connections (Fig 12). At first sight, therefore, the heart seemed to be a classical example of congenitally corrected transposition. On further inspection, however, it was noted that the arterial root that was right-sided and posterior and arose from the right-sided morphologically left ventricle (Fig 13) gave rise to both coronary arteries. The morphologically left coronary artery arose from the anterior and right-sided adjacent arterial sinus (sinus #1) as viewed from the non-adjacent sinus. It gave rise to the anterior interventricular and circumflex arteries, the latter artery extending rightwards to enter the right atrioventricular groove. The morphologically right coronary artery arose from the left-sided adjacent sinus (sinus #2), and passed behind the pulmonary trunk to enter the left-sided atrioventricular groove (Fig 13). The arterial trunk arising from the morphologically left ventricle, therefore, was the aorta, with the pattern of coronary arterial supply typical for left-handed ventricular topology (Fig 12b). A thin rim of myocardial tissue was seen at the base of the root, interposing between the leaflets of the aortic and mitral valves (Fig 12a). There was a perimembranous ventricular septal defect opening directly beneath the aortic root, with its postero-inferior margin formed by fibrous continuity between the leaflets of the mitral and tricuspid valves (Fig 12a). The pulmonary valve was anterior and left-sided (Fig 13), arising from the left-sided morphologically right ventricle above an extensive subpulmonary infundibulum (Fig 12b).

Figure 12 The images show the right-sided ( a ) and left-sided ( b ) ventricles from a heart with usual arrangement of the atrial chambers. The left-sided ventricle is clearly morphologically right and shows left handed topology. The arterial root arising from the right-sided morphologically (morph) left ventricle, however, is the aorta, which is positioned posterior and to the right (see Fig 13). There is a perimembranous ventricular septal defect (star) opening to the outlet of the right ventricle.

Figure 13 The images reveal the right-sided and posterior aortic root from the heart shown in Figure 12. It gives rise to the coronary arteries, showing that it is the aorta. The arrangement of the coronary arteries is typical of left-handed ventricular topology.
In terms of sequential segmental analysis, the heart was from a patient with usual atrial arrangement and discordant atrioventricular, but concordant ventriculo-arterial, connections. The aortic root, however, was posterior and right-sided, which is the expected arrangement in patients with usual atrial arrangement and concordant atrioventricular connections. In the light of the usual atrial arrangement, but with mirror-imaged arrangement of the ventricular mass, this combination could be described by those advocating segmental analysis as “isolated ventricular inversion”.Reference Van Praagh 10 In lesions described in this manner, however, the aortic valvar leaflets, located posteriorly relative to the pulmonary trunk, are expected to be in fibrous continuity with the leaflets of the mitral valve. As can be seen, the heart from this particular patient possesses a small, but complete, sub-aortic infundibulum (Fig 12a), as was also the case in our patient diagnosed clinically but with left-sided location of the aorta (Fig 7). This finding points to the advantages of using the morphological method for analysis, as in both patients the ventriculo-arterial connections were concordant, with parallel arterial trunks, irrespective of the presence or absence of fibrous continuity between the leaflets of the aortic and mitral valves. It would presumably be a judgement call for those wishing to use the segmental approach in determining whether the heart from the patient shown in Figures 12 and 13 had “anatomically corrected malposition” because of the sub-aortic infundibulum or “isolated ventricular inversion” because of the location of the aortic root.
On the other hand, there is a potentially much greater problem to be considered when contemplating the use of the description of “isolated ventricular inversion”. As we have shown in Figure 1, when there are “normal arterial relations”, the right-sided aortic valve has fibrous continuity with the left-sided mitral valve. In the combination identified as so-called “isolated ventricular inversion”, however, the right-sided aortic valve is described as being in fibrous continuity with the mitral valve, which is also right-sided.Reference Van Praagh and Van Praagh 9 This is hardly a “normal relationship”. If the arterial roots occupy their “normal positions” in the setting of left-handed ventricular topology and concordant ventriculo-arterial connections, which will then be mirror-imaged, as we have shown in Figure 2, the aortic root will be left-sided. Its leaflets will be in continuity with the leaflets of the right-sided mitral valve. As we will discuss, this feature becomes more important when considering left-handed ventricular topology with concordant ventriculo-arterial connections in the setting of patients with isomeric atrial appendages, as opposed to those with usual or mirror-imaged atrial chambers. As we have also mentioned, nonetheless, the combination of usual atrial arrangement, discordant atrioventricular connections, and concordant ventriculo-arterial connections is also described as “isolated ventricular discordance”. As judged by a recent description, this is considered by some to be the same entity as “isolated ventricular inversion”.Reference Sharma, Marwah, Shah and Maheshwari 22 Nevertheless, is this necessarily the case? Yet another patient of ours seen recently at the All India Institute of Medical Sciences in New Delhi illustrates well the dilemma in making an appropriate diagnosis.
The patient, who was aged 4 months, was noted to have usual arrangement of the thoraco-abdominal organs including the atrial appendages (Fig 14). The reversed off-setting of the hinges of the atrioventricular valves (Fig 14b) confirmed the presence of discordant atrioventricular connections, but analysis of the ventriculo-arterial junctions showed that the left-sided morphologically right ventricle was giving rise to the pulmonary trunk (Fig 15). The aortic valve arising exclusively from the right-sided morphologically left ventricle was anterior and right-sided relative to the pulmonary valve. In this patient, therefore, with usual atrial arrangement, the atrioventricular connections were discordant, but the ventriculo-arterial connections were concordant. The aortic valve arising anteriorly from the right-sided morphologically left ventricle was supported by a completely muscular infundibulum. For those using segmental analysis, therefore, the patient exhibited the segmental combination of {S,L,D}, which equates to the so-called “anatomically corrected malposition”. As discussed, some might choose to describe the combination as “isolated ventricular discordance”. It would be a mistake, however, to consider the combination as showing “isolated ventricular inversion”, as the segmental arrangement for that entity is {S,D,S}. Thus, although used interchangeably, these two terminologies represent different morphological subsets.Reference Sharma, Marwah, Shah and Maheshwari 22 Such problems in nomenclature by those using the segmental approach are neatly circumvented simply by describing the presence of discordant atrioventricular connections but with concordant ventriculo-arterial connections and parallel arterial trunks.

Figure 14 The echocardiographic images in four-chamber projection show usual atrial arrangement ( a ) and discordant atrioventricular connections. As is shown in panel ( b ), there is reversed off-setting of the hinges of the leaflets of the atrioventricular valves (arrows), showing the left-sided valve to be morphologically (morph.) tricuspid and the morphologically right ventricle (RV) to be left-sided. The star shows the location of a perimembranous ventricular septal defect.

Figure 15 Anterior tilting of the images obtained in four-chamber projection shows that the bifurcating pulmonary trunk is arising from the left-sided morphologically right ventricle (morph RV), with its root overriding a ventricular septal defect (star). The aortic valve, arising from the right-sided morphologically left ventricle, is anterior and right-sided relative to the pulmonary valve ( b ).
Can “isolated ventricular inversion” or “isolated atrial inversion” exist in patients with so-called “visceral heterotaxy”?
It is by no means rare to find concordant ventriculo-arterial connections in the setting of left-handed ventricular topology in patients with so-called “visceral heterotaxy”. In the series of hearts that we have been able to study morphologically, however, these features have mostly been seen when the arterial trunks are spiralling, rather than parallel, as they exit the pericardial cavity (Fig 16). As described above, this is the expected “normal” arrangement of concordant ventriculo-arterial connections when there is left-handed ventricular topology (Fig 2a). The heart shown in Figure 16a was from a foetus with left bronchial isomerism (Fig 16b). The pulmonary veins in this foetus all drained to the right-sided atrium (Fig 16a), with the systemic veins connecting to the left-sided atrium. Both atriums, however, had morphologically left appendages (Fig 17). It would be incorrect, therefore, when considering the heart shown in Figures 16 and 17, to suggest that the atrial arrangement was mirror-imaged, as the concept of the morphological method dictates that structures should be defined on the basis of their intrinsic characteristics and not according to features that are themselves variable, such as the veno-atrial connections. The venous returns are not infrequently lateralised in the setting of isomeric atrial appendages. Even when all the pulmonary veins connect to one atrium, however, and all the systemic venous return is to the other atrium, the morphological method dictates that it should be the morphology of the appendages that is the arbiter of atrial arrangement (Fig 18). In the heart shown in Figures 18 and 19, as in the heart shown in Figures 16 and 17, the atrial arrangement is of left isomerism, despite the presence of seemingly mirror-imaged venous returns. In the heart shown in Figures 18 and 19, there was right-handed ventricular topology, with concordant ventriculo-arterial connections and normally spiralling arterial trunks. Those using a segmental approach would describe the arrangement as “isolated atrial inversion”. The isomeric arrangement of the atrial appendages shows that this would be an incorrect designation. Identifying the atrial arrangement on the basis of the appendages, as dictated by the morphological method, however, is of importance not only for reasons of nomenclature.

Figure 16 Panel ( a ) shows the frontal view of the heart and lungs of a foetus. The heart is right-sided, with the pulmonary trunk moving from right to left as it spirals round the left-sided aortic root. The atrial appendages are both morphologically left, with the bronchial tree, shown in panel ( b ), revealing the features of left isomerism. Both bronchi are long and are crossed by the arteries to the lower lobes of the lungs before they branch.

Figure 17 The images show the right-sided ( a ) and left-sided ( b ) atrial chambers of the heart illustrated in Figure 16. Both are of left morphology. All the pulmonary veins connect to the right-sided atrium ( a ), whereas the systemic veins drain to the left-sided atrium ( b ). The veno-atrial connections, therefore, are mirror-imaged.

Figure 18 The images show the left-sided ( a ) and right-sided ( b ) atrial chambers from a heart taken from a patient with mirror-imaged venous returns (see Fig 19). Both of the appendages are morphologically left. Using the principle of the morphological method, therefore, the patient can be diagnosed as having left isomerism. Note that there are also bilateral superior caval veins (SCV). As can be seen from Fig 19, however, the right-sided caval vein drains to the left-sided atrium. Note the spiralling arterial trunks as well, with the aorta arising from the left ventricle.
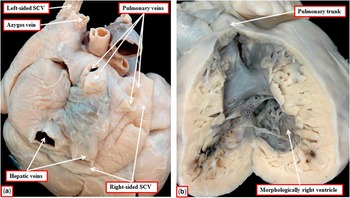
Figure 19 The heart shown in Figure 18 is photographed from the right-side and behind to produce panel ( a ). As can be seen, the right-sided superior caval vein (SCV) enters the right-sided atrioventricular groove. It then drains through the coronary sinus into the left-sided atrium, which also receives the left-sided superior caval vein that drains the venous return from the abdomen through the azygos venous system and both hepatic veins. All four pulmonary veins drain to the right-sided atrium. The venous returns, therefore, are mirror-imaged. The right-sided atrium, however, connects to a morphologically right ventricle ( b ), which gives rise to a normally related pulmonary trunk. If assessed on the basis of venous returns, the patient would be diagnosed as having “isolated atrial inversion”. In fact, the patient has left isomerism, with mixed atrioventricular connections, right-handed ventricular topology, and concordant ventriculo-arterial connections with normally spiralling arterial trunks. Note that there is also so-called non-compaction of the morphologically right ventricle.
When the atrioventricular connections are mixed in the setting of isomeric atrial appendages, then the left-handed ventricular topology is known to be associated with dual atrioventricular nodes, along with a sling of conduction tissue between the connecting atrioventricular bundles.Reference Ho, Fagg, Anderson, Cook and Allan 23 , Reference Smith, Ho, Anderson, Connell, Arnold and Wilkinson 24 In such cases, where the diagnosis is to be made on the basis of the venous returns – namely, that of mirror-imaged atrial arrangement with left-handed ventricular topology – the presumption would then be made that the atrioventricular connections were concordant.Reference Anderson, Brown, Meno and Spicer 25 This would result in a spurious assumption that the atrioventricular conduction tissues are also mirror-imaged, with a regularly positioned but left-sided atrioventricular node. Determining atrial arrangement on the basis of the morphology of the appendages is also important when determining the site of the sinus node, which is present bilaterally with isomeric right appendages, but often hypoplastic and difficult to locate when there are isomeric left appendages.Reference Ho, Fagg, Anderson, Cook and Allan 23 , Reference Smith, Ho, Anderson, Connell, Arnold and Wilkinson 24
Comment
In the mid-20th century, despite several previous descriptions,Reference Harris and Farber 1 the very existence of hearts with concordant ventriculo-arterial connections, but with the aorta arising anteriorly from the morphologically left ventricle, had been doubted on the grounds that such an arrangement was an embryological impossibility.Reference Van Mierop and Wiglesworth 2 When it became evident that such combinations did indeed exist,Reference Van Praagh and Van Praagh 3 the focus of attention in such lesions shifted from discussions of embryology to debates concerning nomenclature. This was because, until the mid-20th century, many held the view that an anterior aorta, supported by a completely muscular infundibulum, was the defining feature of “transposition”.Reference Van Mierop 4 Therefore, if the aorta was arising anteriorly from the morphologically left ventricle, it had to be anatomically corrected.Reference Harris and Farber 1 It subsequently became accepted that the essence of “transposition” was the presence of discordant ventriculo-arterial connections, as it had been shown that the aorta could itself be “normally related” to the pulmonary trunk, despite arising from the morphologically right ventricle.Reference Van Praagh 5 As it then became obvious that, in this sense, an anterior aorta arising from the left ventricle was not “transposed”, the arrangement of concordant ventriculo-arterial connections, but with parallel arterial trunks, was re-named as anatomically corrected malposition.Reference Kirklin, Pacifico, Bargeron and Soto 6
Although the use of “anatomically corrected malposition” was certainly an improvement over the previous label of “anatomically corrected transposition”, the revised term does little to instruct the reader about either the physiological or anatomical aspects of this rare anomaly. This is because “malposition” is now used more frequently to describe the relationship of the aorta with the pulmonary trunk when both arterial trunks arise from the morphologically right ventricle.Reference Van Praagh 10 The situation is then more complicated, as the combination of concordant ventriculo-arterial connections with parallel arterial trunks can be found in association with all varieties of atrial arrangement and with varied atrioventricular connections.Reference Anderson, Becker, Losekoot and Gerlis 7 Those most vocal in promulgating the term “anatomically corrected malposition”,Reference Van Praagh 10 furthermore, require that the aortic valve, when arising abnormally from the morphologically left ventricle, be supported by a completely muscular infundibulum. This is because, in the notations used to account for the variants of segmental anatomy,Reference Van Praagh 10 the arrangement in which the aortic root is positioned posteriorly and leftward relative to the pulmonary root is considered to be the mirror-image of the pattern found in the normal heart, but only when there is fibrous continuity between the leaflets of the aortic and mitral valves.
This means that in the setting of usual atrial arrangement patients are labelled as having “isolated ventricular inversion”Reference Van Praagh 10 or alternately “isolated ventricular discordance” when the atrioventricular connections are discordant, the ventricular topology is left-handed, the ventriculo-arterial connections are concordant, and the aortic root is positioned posteriorly and rightward, with fibrous continuity between the leaflets of the right-sided aortic and mitral valves. As we have shown, however, this anatomical arrangement of the aortic and mitral valves, considered comparable with the normal arrangement by those defining segmental anatomy, is not directly analogous to the situation encountered in the normal heart. In the normal arrangement, the leaflets of the aortic valve are in fibrous continuity with the left-sided mitral valve (Fig 1). As we have also shown, some use the term “isolated ventricular inversion” when the arrangement should properly be considered to represent “anatomically corrected malposition”. In either event, it is inappropriate to consider the situation in which the aortic valvar leaflets are in continuity with the leaflets of the right-sided mitral valve as representing normality. Furthermore, in the situation as shown in one of our anatomical specimens (Fig 12a), a small rim of myocardium can separate the leaflets of the aortic and mitral valves, despite the fact that the aortic root is positioned posteriorly and rightward relative to the subpulmonary infundibulum. Does the presence of this small rim of muscle mean that the proponents of segmental anatomyReference Van Praagh 10 would label the heart as showing “anatomically corrected malposition” rather than “isolated ventricular discordance”?
The situation concerning the naming of such rare entities becomes further complicated when it is appreciated that all of these features can be seen in mirror-imaged atrial arrangement or when the atrial appendages are isomeric rather than lateralised. When the atrial chambers are mirror-imaged, but the atrioventricular connections are discordant, the ventricular mass typically shows right-handed topology. In this setting, therefore, the relationship of the ventricles is analogous to that seen in the normal heart and in the majority of patients with congenitally malformed hearts. Owing to this fact, those wishing to use specific titles are forced to describe “isolated ventricular non-inversion”.
All these considerations illustrate the ongoing problems that exist as we seek to establish a universally acceptable nomenclature for congenitally malformed hearts. In our opinion, for all the reasons we have identified, it does not help to use such arcane phrases such as “anatomically corrected malposition”, “isolated ventricular discordance”, “isolated ventricular non-inversion”, or “isolated infundibuloarterial discordance” to describe these very rare entities.Reference Van Praagh and Van Praagh 9 , Reference Van Praagh 10 We submit that it is far more sensible, in these unusual circumstances, to take the time to describe first the ventriculo-arterial and atrioventricular connections, then the relationships of the arterial roots, and finally the specific infundibular morphologies.Reference Anderson and Ho 11 , Reference Anderson and Shirali 12 , Reference Cavalle-Garrido, Bernasconi, Perrin and Anderson 14 When considering the feature of aortic-mitral continuity, it is also crucial to consider this feature in the setting of the ventricular topology, rather than on the basis of the relationship of the arterial roots. The diagnostic techniques currently available during life permit each of these features to be demonstrated with exquisite accuracy. Indeed, the advent of techniques such as computed tomographic angiography now demonstrate the anatomy during life with just as much precision as is available during autopsy. It is the advances in diagnostic imaging as much as anything that call for a re-appraisal of terminology. In the days when segmental analysis was first established, it was not possible with certainty to determine either the connections between the cardiac segments or the specific morphology of the arterial roots. Owing to these technical shortcomings, it was often necessary to infer the connections present from the information available regarding arterial relationships. As we have shown, this is no longer necessary. Therefore, we now need to match the advances in imaging with the terms we use to describe the findings. This means that things should be described in a simple and straightforward manner, taking time to account for all the abnormalities encountered. Only in this way will we do justice to the fact that the modern-day paediatric cardiologist can image the heart with just as much accuracy as the morphologist working in the autopsy room.



















