



A 5-month-old baby was referred to our hospital due to status epilepticus with hemispherectomy. He was intubated due to increasing seizure activity. Placement of a central venous line via a right subclavian approach was attempted using the landmark technique. Following insertion of the guide wire, we attempted to advance a catheter over the guide wire. The catheter was unable to be advanced due to resistance and was removed. We encountered difficulty removing the guide wire, reluctant to use excessive force due to the risk of tearing the vessel. A bedside X-ray showed a kinked or knotted guide wire at the level of the right clavicular head and interval collapse of the right upper lobe (Fig 1). Hence, it was decided to remove the guide wire surgically as well as place a secure central venous line.
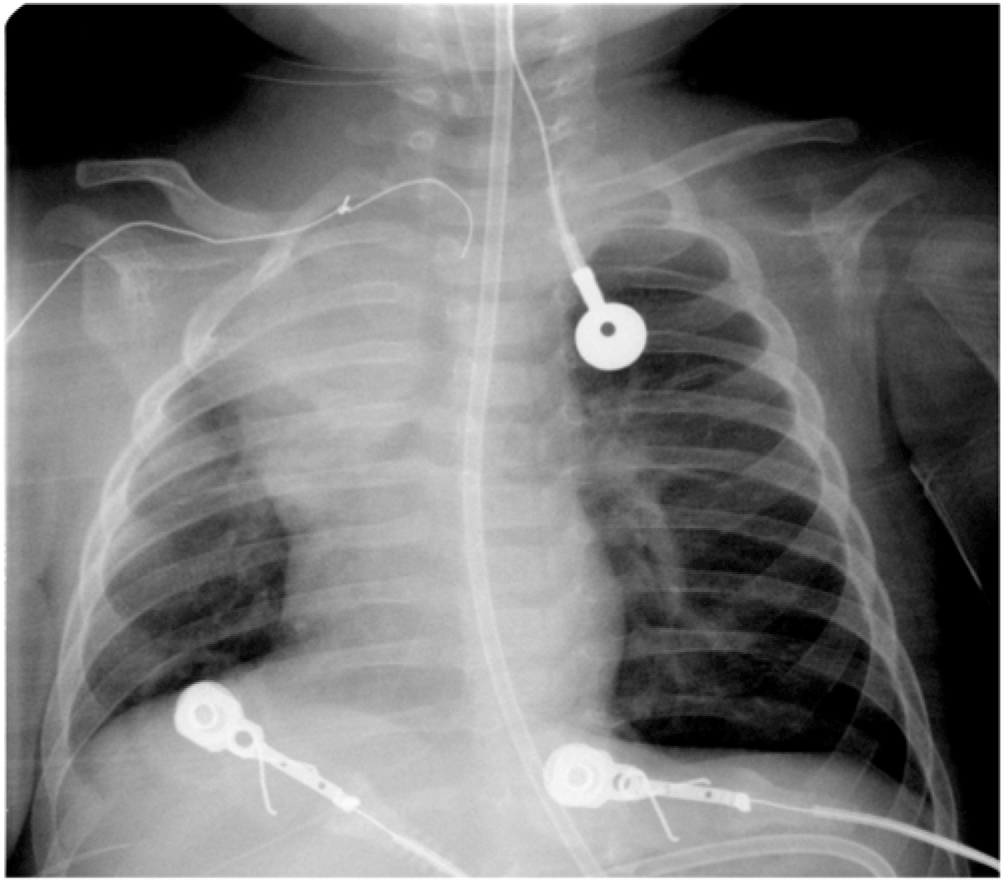
Figure 1. A bedside chest X-ray.
A Broviac catheter was inserted into the left subclavian vein under fluoroscopy before exploration of the right subclavian guide wire. Through a subclavicular incision, the guide wire was found to have passed through the subclavian vein just distal to its confluence with the jugular vein. It exited the back wall of the subclavian vein and entered the innominate artery. A venotomy and arteriotomy were required to extract the guide wire from the vessels without significant bleeding (Fig 2). The patient underwent hemispherectomy on day 2 and went home on day 19 postoperatively.

Figure 2. Removed guide wire.
This event and accompanying images represent a rare complication of central venous catheter placement and highlight the risks involved in placing central venous catheters.
Acknowledgements
None.
Financial Support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflicts of Interest
None.
Ethical Standards
The research does not involve human and/or animal experimentation.


