


Involvement of the cardiovascular system in chronic kidney disease is an important cause of morbidity and mortality. While renal dysfunction progresses, cardiac function irreversibly deteriorates. Cardiovascular complications are responsible for 28–32% of deaths, especially in dialysed children. 1 Abnormal left ventricular geometry resulting in dysfunction is associated with poor cardiovascular prognosis in patients with chronic kidney disease.Reference Mclntyre, Odudu and Eldehni 2
Conventional transthoracic echocardiography is a non-invasive method that provides information about left ventricle structure and function. However, left ventricle ejection fraction and shortening fraction seem to be close to normal even in end-stage renal disease.Reference Mclntyre, Odudu and Eldehni 2 Myocardial function can be evaluated in more detail by 2D-Speckle Tracking Echocardiography, consisting of two-dimensional myocardial deformation analyses based on continuous monitoring of the movement of natural acoustic markers (speckles), which are characteristics of the myocardium. It also allows examination of the heart movements in the longitudinal, radial, and circumferential dimensions. The advantages of this method are that it is angle-independent, less load-dependent, easier to analyse and interpret compared with tissue Doppler imaging, and has less variability between different echocardiographers or the same echocardiographer at different times.Reference Blessberger and Binder 3 , Reference Yan, Li and Hao 4 With the help of the technique, sub-clinical myocardial infarction in patients with chronic kidney disease can be demonstrated earlier.Reference Edwards, Hirth, Ferro, Townend and Steeds 5 In the literature, there are a few studies on 2D-speckle tracking echocardiography imaging techniques in adult patients with chronic kidney disease; however, it has not been studied during the stages of the disease or with respect to age as cardiac impairment is first seen in children. Thus, the aim of the study was to assess regional myocardial systolic and diastolic functions by using 2D-speckle tracking echocardiography in children with chronic kidney disease having preserved left ventricle ejection fraction.
Materials and methods
The study included 38 patients aged 6–18 years. Patients with the diagnosis of chronic kidney disease having a glomerular filtration rate of <90 ml/minute/1.73 m2 for at least 3 months were followed up at a paediatric nephrology clinic between January 2013 and December 2015. Stages of patients were determined according to Hogg’s classification.Reference Hogg, Furth and Lemley 6 The control group included 37 healthy children with similar age and gender who were referred to the paediatric cardiology clinic with an innocent murmur or nonspecific chest pain. Patients with renal transplantation or acute renal failure were excluded from the study. Other exclusion criteria in the study were having abnormal wall movements of the heart, low ejection fraction (<60%), arrhythmia, obesity (body mass index >35 kg/m2), sub-optimal image quality, congenital or acquired heart disease, and other systemic diseases. Anthropometric measurements, heart rate, arterial blood pressure, and 12-lead electrocardiography of the patients were recorded. Glomerular filtration rate of children with chronic kidney disease was calculated by the Schwartz formula. The local Ethics Committee (2013/242) approved the study, and all subjects provided informed consent.
Echocardiographic evaluation
Echocardiographic evaluation was performed in left lateral position, in expiration, in a quiet environment without sedation using a Vivid S5 echocardiography device and a 3S-RS probe (3.5 MHz) (GE Vingmed, Horten, Norway). Images were taken in apical long-axis and parasternal short-axis positions in 2D and M-mode. Ejection fraction and shortening fraction were measured by modified Simpson’s biplane method in apical four-chamber view by scanning the endocardial surface.Reference Cain, Ahl and Hedstrom 7 , Reference Tumuklu, Etikan, Kisacik and Kayikcioglu 8 Shortening fraction was calculated by M-mode echocardiography as in the formula (left ventricular end-diastolic dimension – left ventricular end-systolic dimension)/left ventricular end-diastolic dimension×100. Left atrial dimension at end-systole was measured from the outer edge of the posterior aortic wall to the endocardial surface of the posterior wall of left atrium, and aortic root diameter at end-diastole was measured from the outer edge of the anterior wall to the outer edge of the posterior wall in apical long-axis view by M-mode echocardiography. Next, the left atrium/aorta ratio – increased left atrium/aorta ratio means left atrial dilatation is present – was calculated. Left atrial volume at the end-ventricular systole and left ventricle end-diastolic volume were calculated with modified Simpson method as well.
In the parasternal long-axis M-mode echocardiographic evaluation, left ventricular end-diastolic diameter, left ventricular end-systolic diameter, left ventricular diastolic posterior wall thickness, and interventricular septum thickness values were measured. Left ventricle mass was calculated by Devereux and Reishek formula by using these values.Reference Devereux and Reichek 9 Left ventricular mass index was found by dividing the left ventricular mass by body surface area.
The sample volume was set to the edges of the mitral valve, with pulse wave Doppler to the left ventricular inflow region, and the direction of the Doppler wave was set parallel to the blood flow in the apical four-chamber view. Mitral early filling (e) and late filling (a) peak velocities, e/a ratio, and mitral e-wave deceleration time were measured. Tricuspid annular plane systolic excursion was measured by M-mode through an apical four-chamber view.
2D-speckle tracking echocardiography
Standard echocardiographic images were obtained in the apical four-chamber, apical two-chamber, and apical long-axis and short-axis planes at the papillary muscle level of the mitral valve, and three consecutive end-expiratory cardiac cycles were acquired. For short-axis left ventricle analyses, the cross-sectional image was as circular as possible.
Data from three cardiac cycles were averaged and offline statistical analysis was performed using EchoPAC software (version 8.0, GE healthcare PC 2008, Boston, Massachusetts, United States of America). After initialising three points on an end-diastolic frame on the mid-myocardium in each long-axis image or initialising the midpoint of the interventricular septum in each short-axis image, the software automatically divided the left ventricle myocardium into six segments and performed speckle tracking analysis in the regions throughout the cardiac cycle. Manual adjustments of tracking points were performed when needed. Finally, data were exported to a spreadsheet program (Excel; Microsoft Corp., Redmond, Washington, United States of America) to determine regional motion and deformation of lateral and septal walls of the left ventricle at basal, medial, and apical segments. The longitudinal strain and longitudinal strain rate – systolic, early diastolic, and late diastolic – averages of six regions were obtained in two-, three-, and four-chamber views. Radial strain and radial systolic strain rates – early diastolic and late diastolic – and circumferential strain and circumferential systolic strain rates – early diastolic and late diastolic – were measured at the papillary muscle level of the mitral valve in the parasternal short-axis view. Early strain rate was divided by late diastolic strain rate to obtain the strain rate e/a ratio. Averages of obtained data were compared in patient and control groups. An example for 2D-speckle tracking echocardiography is shown in Figure 1.
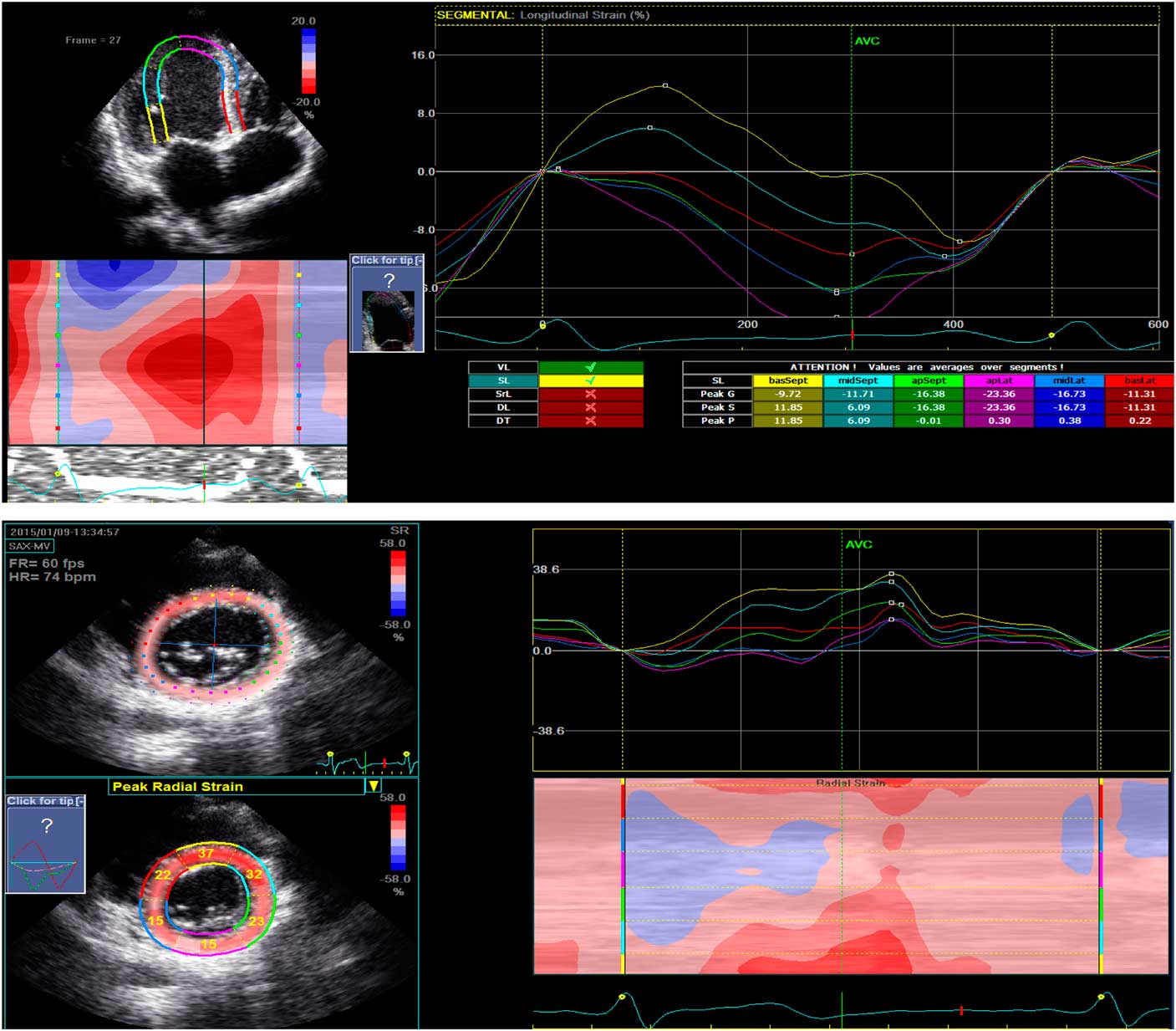
Figure 1 An example for 2D-speckle tracking echocardiography imaging. ( a ) Longitudinal strain image in apical long-axis and four-chamber views. ( b ) Radial strain image in the parasternal short axis at the level of the mitral valve.
Statistical analysis
The data were processed and analysed using the SPSS/16 statistical package. Data were analysed by using descriptive statistical methods – mean, standard deviation, frequency, ratio, minimum, and maximum values. Mann–Whitney U-test and/or Student’s t-test were used for the analysis of the independent variables in both groups according to the distribution. Significance was considered as p<0.05.
Results
The study included 38 patients with chronic kidney disease and 37 healthy controls who had appropriate echocardiographic images. Among the patients, 15 were on regular haemodialysis or peritoneal dialysis, whereas 23 were not. A total of 16 patients were treated with antihypertensive drugs; the remaining 22 were not. Three patients were in stage II chronic kidney disease, ten patients were in stage III, seven patients were in stage IV, and three patients were in stage V. There were no significant differences in age, gender, and weight and body mass index between the patient and control groups. The mean height of the patients with chronic kidney disease was lower than the control group (p=0.03).
In the patients, mean left ventricular mass index was significantly higher than the controls (p<0.05). Systolic and diastolic blood pressure values of the patients were also significantly higher than controls, but the mean heart rates were similar. Haemoglobin values were significantly lower in the patient group, whereas calcium and phosphorus levels were significantly higher (Table 1).
Table 1 Demographic and clinical characteristics of patient and control groups.

ARB=angiotensin receptor blocker; BMI=body mass index; Ca Ch. Blocker=calcium-channel blocker; DBP=diastolic blood pressure; Hb=haemoglobin; LVMI=left ventricular mass index; SBP=systolic blood pressure
There was no significant difference in mitral e value, mitral a value, mitral e/a ratio, mitral deceleration time, and left atrium/aorta ratios between the groups. Furthermore, end-diastolic and end-systolic diameter values of the left ventricle were similar between the groups. However, tricuspid annular plane systolic excursion values of the patient group were significantly lower than those in the control group (p<0.01). The evaluation of the conventional echocardiographic parameters of the groups is shown in Table 2.
Table 2 Echocardiographic parameters of the patient and control groups.

EF=ejection fraction; LA/Ao=left atrium/aorta ratio; LVEDD=left ventricular end-systolic diameter; LVEDS=left ventricular end-diastolic diameter; Mitral a=left ventricular late filling peak velocity; Mitral DT=mitral valve deceleration time; Mitral e=left ventricular early filling peak velocity; Mitral e/a=mitral early filling peak velocity/late filling peak velocity; SF=shortening fraction; TAPSE=tricuspid annular plane systolic excursion
Longitudinal peak systolic strain values in apical long axis were lower in the patient group, and values were statistically significant in the three-chamber and two-chamber views (Table 3).
Table 3 Longitudinal global strain values in apical 4-chamber, 3-chamber, and 2-chamber views.

Longitudinal, radial, and circumferential peak systolic strain values were lower in the patient group, but this difference was statistically significant only in the measurements of all three segments of longitudinal and the circumferential basal segment (p<0.05). The values of radial and circumferential systolic strain rate in all three segments were significantly lower in the patient group (p<0.05). Although longitudinal systolic strain rates of all segments were lower in the patients, the difference was not statistically significant (p>0.05). Moreover, early diastolic strain rate was significantly lower in the apical segments of longitudinal and radial measurements and in all segments of circumferential measurements in the patients. There was no significant difference between groups in all segments of late diastolic strain rate values (p>0.05). However, the strain rate e/a ratio was significantly lower in all segments in longitudinal measurements in the patients (p=0.01) (Table 4).
Table 4 Strain and strain rate values of the groups measured by 2D-speckle tracking echocardiography.

*p<0.05
On the basis of Hogg’s classification, patients in the early – the first, second, and third – stages of chronic kidney disease were compared with the more advanced fourth and fifth stages of the disease: no significant differences were found with respect to ejection fraction, shortening fraction, mitral e, mitral a, and mitral e/a ratios. However, there was an increase in left atrium/aorta ratio and a decrease in tricuspid annular plane systolic excursion values parallel to glomerular filtration rate decline, although not statistically significant. Mitral e, mitral a, and mitral e/a values in patients receiving dialysis and those not receiving dialysis were similar.
Discussion
The time of onset of cardiac effects in children with chronic kidney disease and its progression remain unclear. In patients with chronic kidney disease, metabolic abnormalities, problems caused by volume overload, cardiomyopathy caused by uraemia, and calcium and phosphorus imbalance can lead to the development of myocardial fibrosis. It would be advantageous to identify patients with evidence of cardiac dysfunction early to commence therapy that could minimise further cardiac deterioration.Reference Rakhit, Zhang, Leano, Armstrong, Isbel and Marwick 10 For these patients, it has been shown that heart damage cannot be recognised early enough with the available laboratory studies. Rinat et al has showed elevated levels of serum B-type natriuretic peptide and NT-pro brain natriuretic peptide in patients with advanced stages of renal insufficiency. Moreover, they have reported that the elevation of the peptides disappeared under dialysis. They have also emphasised troponin as a possible marker of cardiac death but not myocardial damage.Reference Rina, Cohen and Nir 11 When cardiac damage was evaluated by conventional echocardiographic methods, ejection fraction and shortening fraction did not adequately reflect regional systolic function that usually seems almost normal by the end stages of the disease.Reference Hayashi, Brodin and Alvestrand 12 As these parameters are load-dependent, it is worth showing sub-clinical effects with tissue Doppler imaging, which measures the direct movement of heart muscle. On the other hand, 2D-speckle tracking echocardiography is a more recent echocardiographic assessment method that can show earlier cardiac effects in patients with chronic kidney disease in the presence of preserved ejection fraction. There are a number of publications in the literature that have used 2D-speckle tracking echocardiography in adults to demonstrate regional left ventricular dysfunction.Reference Altekin, Kucuk and Yanıkoglu 13 – Reference Liu, Su and Huang 16 Liu et al has reported that left ventricular ejection fraction reflected the sum of regional movements of the left ventricle and remained unchanged until several segments were effected in these patients. They also stated that the deterioration of renal function was correlated with the decrease in left ventricular longitudinal peak systolic strain, circumferential strain, and strain rate, reflecting systolic dysfunction.Reference Liu, Su and Huang 16 Yan et alReference Yan, Li and Hao 4 found that peak systolic velocities decreased in the longitudinal basal and apical segments and in the radial basal segment in patients with chronic kidney disease. In our study, the peak systolic strain values were significantly lower in longitudinal and some circumferential segments in the patient group. Similarly, systolic strain rate values in radial and circumferential views were also significantly lower in patients. This might suggest that there was a systolic sub-clinical effect in patients with chronic kidney disease with preserved ejection fraction.
Although diastolic dysfunction is associated with cardiovascular mortality in patients with chronic kidney disease, diastolic function is usually preserved until the late stages of the disease, similar to systolic function.Reference Otsuka, Suzuki, Yoshikawa and Sugi 17 – Reference Kjaergaard, Akkan, Iversen, Kober, Torp-Pedersen and Hassager 20 It has also been shown that radial and circumferential diastolic functions are preserved up to advanced disease stages, whereas longitudinal diastolic dysfunction begins earlier.Reference Otsuka, Suzuki, Yoshikawa and Sugi 17 , Reference Gibson and Francis 18 Parallel with the literature, we found that there was no significant difference between patient and control groups with respect to early/late diastolic strain rate e/a ratio in short-axis radial and circumferential views. In our study, although there was no significant difference in the mitral e/a ratio, the early/late diastolic strain rate ratio in all segments in the longitudinal view as measured by 2D-speckle tracking echocardiography was significantly lower in the patient group. This result suggests that 2D-speckle tracking echocardiography may be a promising investigation for the early recognition of diastolic heart failure in children with chronic kidney disease. Moreover, this imaging modality may motivate clinicians to instigate dialysis earlier in patients with chronic kidney disease with preserved ejection fraction, which may lead to a decrease in mortality and morbidity.
In a study of hypertensive adult patients, the development of cardiac fibrosis caused by collagen accumulation resulted in both systolic and diastolic dysfunctions. It has also been reported that there was a relationship between the progressive increase in serologic markers and the development of fibrosis with a progressive decrease in left ventricle longitudinal peak systolic strain and strain rate.Reference Plaksej, Kosmala and Frantz 21 Our results also suggest that the decrease in strain and strain rate may be helpful in the early demonstration of diastolic dysfunction, as well as left ventricular systolic dysfunction caused mainly by cardiac fibrosis. Another important result of our study was early diastolic strain rate values being significantly lower in the apical segments of longitudinal two- and three-chamber views, and apical segments of radial and circumferential short-axis views in the patients. It is assumed that even if the disease is not global regional diastolic impairment starts earlier and that the function of the heart both in the short and long axes is affected.
Tricuspid annular plane systolic excursion is usually a parameter used to indicate right heart systolic impairment, but there are also studies showing that in some cases there is a decrease in tricuspid annular plane systolic excursion when the left ventricle is affected.Reference Kosmala, Plaksej and Strotmann 22 , Reference Ereminiene, Vaskelyte and Stoskute 23 Akkaya et alReference Akkaya, Erdoğan, Sağ, Arı, Türker and Yılmaz 24 have shown that not only the left heart but also the right heart was affected, and functional failure could be seen in patients with chronic kidney disease. In our study, similarly, tricuspid annular plane systolic excursion values were significantly lower in patients with chronic kidney disease, so it can be considered that the right heart was also affected.
Moreover, the wall motion abnormality of the heart is more prominent in adult patients with chronic kidney disease, where 2D-speckle tracking echocardiography imaging has been studied frequently. Thus, definitive cut-off points have been determined in this population and this technique is used in daily practice. However, in the paediatric population, such studies are small in number and need to have standardisation.
The most important limitation of the study is the small number of cases for comparison of receiving or not receiving dialysis, as well as finding no apparent effect of dialysis treatment on 2D-speckle tracking echocardiography measurements.
In summary, in this study, peak systolic strain, systolic strain rate, and early/late diastolic strain rate ratio were lower in children with chronic kidney disease on 2D-speckle tracking echocardiography examination. It has been shown that 2D-speckle tracking echocardiography may have an additional benefit for the early detection of regional systolic and diastolic dysfunctions, especially in patients with chronic kidney disease whose ejection fraction is >50% where there is no evidence of left ventricular dysfunction by conventional echocardiography. However, in order to demonstrate the efficacy of the 2D-speckle tracking echocardiography method in children with chronic kidney disease, further studies within larger populations of children are required.
Acknowledgements
None.
Financial Support
This research received no specific grant from any funding agency or from commercial or not-for-profit sectors.
Conflicts of Interest
None.
Ethical Standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008, and has been approved by the institutional committees of Mersin University.





