


Introduction
Being unable to exert control over one's thoughts when it is perceived to be important has been proposed to be central to understanding several different anxiety disorders, and especially in Obsessive Compulsive Disorder (OCD), where the experience of having particular intrusive thoughts is appraised negatively. Although OCD often starts in childhood (Rasmussen and Eisen, Reference Rasmussen and Eisen1990), little research has explored control of unwanted or intrusive thoughts in this age group. This study aims to explore thought control strategies in young people, and to examine whether they are associated with OCD symptoms and meta-cognitive beliefs.
The cognitive-behavioural models that have been developed for adult OCD have started to be explored in childhood and adolescence (see Cartwright-Hatton, Reynolds and Wilson, Reference Cartwright-Hatton, Reynolds, Wilson, Silverman and Field2011; Reynolds and Reeves, Reference Reynolds and Reeves2008), but to date only very limited research has explored the thought control strategies children and adolescents use to manage their unwanted thoughts and worries (Gosselin et al., Reference Gosselin, Langlois, Freeston, Ladouceur, Laberge and Lemay2007; Laugesen, Dugas and Bukowski, Reference Laugesen, Dugas and Bukowski2003). Farrell and Barrett (Reference Farrell and Barrett2006), in a study of one thought control strategy, thought suppression, found that children with OCD reported significantly less tendency to suppress thoughts in comparison to adults, with the adolescent group not differing significantly from either group. It is therefore interesting that Gaskell, Wells and Calam (Reference Gaskell, Wells and Calam2001) failed to show rebound effects of thought suppression in an experimental study of non-referred 7–11 year olds. It may be that perceived control of thoughts only becomes important in adolescence when there are improvements in meta-cognitive skills (Klaczynski, Reference Klaczynski, Jacobs and Klaczyniski2005). Alternatively, it may be that it is only in later adolescence that cognitive and affective processes are sufficiently co-ordinated for thought control strategies to be reliably effective (Steinberg, Reference Steinberg2008). However, studies of thought control in adolescent OCD have only explored thought suppression and it is possible that other thought control strategies are relevant. In particular, the heightened sensitivity to social-emotional stimuli that is characteristic of early adolescence (Casey, Getz and Galvan, Reference Casey, Getz and Galvan2008) might indicate that the use of strategies involving social control is somewhat different between adolescents and adults.
Motivation to control thoughts may be influenced by a number of factors, such as beliefs about thought control, the meaning of the thought itself, and by beliefs about potential consequences of not controlling the thought (Purdon, Reference Purdon1999). These meta-cognitive factors are robustly associated with OC symptoms in adults (Clark, Reference Clark2004), and indeed several studies have explored the role of young people's cognitive and meta-cognitive beliefs in relation to emotional disorders (Bacow, Pincus, Ehrenreich and Brody, Reference Bacow, Pincus, Ehrenreich and Brody2009; Cartwright-Hatton et al., Reference Cartwright-Hatton, Mather, Illingworth, Brocki, Harrington and Wells2004; Wilson et al., Reference Wilson, Budd, Chernin, King, Leddy, Maclennan and Mallandain2011). Barrett and Healy (Reference Barrett and Healy2003) explored different cognitive factors that form the basis of cognitive-behavioural models of OCD in adulthood, such as thought action fusion, and responsibility beliefs. They found that several cognitive factors did distinguish children with OCD and non-referred children, but only poor cognitive control distinguished children with OCD from children with other anxiety disorders. However, they did not recruit adolescents in this study. Three studies (Cartwright-Hatton et al., Reference Cartwright-Hatton, Mather, Illingworth, Brocki, Harrington and Wells2004; Mather and Cartwright-Hatton, Reference Mather and Cartwright-Hatton2004; Matthews, Reynolds and Derisley, Reference Matthews, Reynolds and Derisley2007) have explored associations between meta-cognitive beliefs and OC symptoms in adolescents using the MCQ Adolescent version (MCQ-A; Cartwright-Hatton et al., Reference Cartwright-Hatton, Mather, Illingworth, Brocki, Harrington and Wells2004). These studies found that all five sub-scales of the MCQ-A – uncontrollability and danger beliefs, superstition, punishment and responsibility beliefs, cognitive self-consciousness, cognitive confidence and positive beliefs about worry – correlated with OC symptoms (Cartwright-Hatton et al., Reference Cartwright-Hatton, Mather, Illingworth, Brocki, Harrington and Wells2004; Matthews et al., Reference Matthews, Reynolds and Derisley2007). Furthermore, MCQ-A total score accounted for independent variance in OC symptoms (Mather and Cartwright-Hatton, Reference Mather and Cartwright-Hatton2004; Matthews et al., Reference Matthews, Reynolds and Derisley2007). Research has not yet addressed whether particular meta-cognitive factors account for independent variance in OC symptoms in adolescents.
The research on thought control in adults is far advanced compared to the research on thought control in young people. Much of this has focused on thought suppression (see Purdon, Reference Purdon1999 for a review), but Wells and Davies (Reference Wells and Davies1994) identified five different types of thought control strategies that are commonly reported by people with anxiety disorders: distraction, social control, worry, punishment and reappraisal. The reported use of these different strategies has been measured in adults with a variety of disorders including OCD, GAD, insomnia, schizophrenia, acute stress disorder and depression (Amir, Cashman and Foa, Reference Amir, Cashman and Foa1997; Coles and Heimberg, Reference Coles and Heimberg2005; Harvey, Reference Harvey2001; Morrison and Wells, Reference Morrison and Wells2000; Warda and Bryant, Reference Warda and Bryant1998; Watkins and Moulds, Reference Watkins and Moulds2009). It appears that the use of punishment and worry to manage unwanted thoughts appears to best distinguish people with psychological disorders from their healthy counterparts (Fehm and Hoyer, Reference Fehm and Hoyer2004; Wells, Reference Wells and Clark2005).
The research is also advanced with respect to meta-cognition in adult OCD. Meta-cognitions have been found to predict OC symptoms experimentally (Fisher and Wells, Reference Fisher and Wells2005) and prospectively (Myers, Fisher and Wells, Reference Myer, Fisher and Wells2009), and changes in meta-cognitions have been found to predict the outcome of therapy (Solem, Håland, Vogel, Hansen and Wells, Reference Solem, Håland, Vogel, Hansen and Wells2009). Two studies have directly tested associations between thought control strategies and meta-cognitions (Moore and Abramowitz, Reference Moore and Abramowitz2007; Tolin, Worhunsky, Brady and Maltby, Reference Tolin, Worhunsky, Brady and Maltby2007). The strategies of worry and punishment were found to be associated with a variety of obsessive–compulsive beliefs including responsibility and threat estimation, perfectionism and certainty, and the importance of and control of thoughts, with other thought control strategies not being associated with OC beliefs. Furthermore, these obsessive-compulsive beliefs mediated the relationship between OC symptoms and punishment in both non-clinical (Moore and Abramowitz, Reference Moore and Abramowitz2007) and clinical (Tolin et al., Reference Tolin, Worhunsky, Brady and Maltby2007) adult participants. The role of meta-cognitions as mediators between thought control strategies and OC symptoms has not been tested in adolescents. In addition, although there are associations between different obsessive-compulsive beliefs that act as mediators, these have yet to be tested as simultaneous mediators in a multiple mediator model.
The aim of the current study was therefore to explore cognitive factors that have been found to be important in cognitive-behavioural models of adult OCD. The current study asked adolescents to report on the different thought control strategies they use to try and control their unwanted thoughts and to test whether these are associated with meta-cognitive beliefs and obsessive-compulsive disorder symptoms. We hypothesized that adolescents would report using a variety of thought control strategies with no significant differences found between mean scores on the Thought Control Questionnaire (TCQ) in our sample and those published in Wells and Davies (Reference Wells and Davies1994) for an adult sample. We hypothesized that the strategies of worry and punishment and a range of meta-cognitive beliefs would be associated with OCD symptoms. Finally, we hypothesized that meta-cognitive beliefs would mediate the relationships between thought control strategies and OC symptoms.
Method
Participants
A non-clinical predominately “White British” (89%) adolescent sample was recruited through schools. Participants included 66 male and 85 female students aged 13–16 years old (M = 15.05, SD = 1.03). Adolescents with special educational needs that might impact upon their ability to complete the measures were not invited to take part and for ethical reasons adolescents who were currently receiving therapeutic treatment for a mental health problem, or had done in the past year, were asked not to return their consent form, and thus were excluded.
To test the first hypothesis, data from the adult sample recruited for the validation study were used. This comprised 96 male and 133 female undergraduate and postgraduate students aged between 18 and 47 years (see Wells and Davies, Reference Wells and Davies1994).
Measures
Thought Control Questionnaire (TCQ; Wells and Davies, Reference Wells and Davies1994). The TCQ is a 30-item self-report questionnaire designed to assess the strategies people use to control unpleasant or unwanted thoughts. Each item is rated on a 4-point rating scale. As well as a total score, the TCQ measures five factors with six items corresponding to each factor. These subscales include distraction, social control, worry, reappraisal and punishment. The scale has good psychometric properties (Wells and Davies, Reference Wells and Davies1994). In the current study the internal consistency was considered acceptable (.63 < α < .79).
Meta-Cognitions Questionnaire – Adolescent version (MCQ-A; Cartwright-Hatton et al., Reference Cartwright-Hatton, Mather, Illingworth, Brocki, Harrington and Wells2004). The MCQ-A is a 30-item self-report questionnaire designed to measure beliefs about worry and intrusive thoughts in adolescents aged 13–17 years. Items are rated on a 4-point scale. As well as a total score the MCQ-A measures five factors with six items corresponding to each subscale; positive beliefs (PB), uncontrollability and danger beliefs (UCD), cognitive confidence (CC), superstition, punishment and responsibility beliefs (SPR) and cognitive self-consciousness (CSC). The scale has good psychometric properties (Cartwright-Hatton et al., Reference Cartwright-Hatton, Mather, Illingworth, Brocki, Harrington and Wells2004).
Leyton Obsessional Inventory – Child Version (Berg, Whitaker, Davies, Flament and Rapoport, Reference Berg, Whitaker, Davies, Flament and Rapoport1988). The LOI –CV is a 20-item self-report inventory designed to assess the frequency of obsessive-compulsive symptoms and the interference (rated 1–4 for each symptom) caused by symptoms in young people aged 8 to 18 years old. It has good psychometric properties (Berg et al., Reference Berg, Whitaker, Davies, Flament and Rapoport1988).
Procedure
Ethical approval for the study was granted by the University Ethics Committee. Information sheets and consent forms were sent out through schools. When both parental and adolescent written consent was obtained, participants attended a session in school to complete the three measures. These sessions were facilitated by the first author and a teacher at the school, in order to answer any questions and to deal with any distress that arose. Information was sent out to 1145 children and 151 returned questionnaires, representing a 13% response rate.
Analysis plan
Several of the variables were not normally distributed and transformations were not successful, and therefore a number of strategies were used to test whether correlation and regression were appropriate analyses. Non-parametric correlations were compared with parametric correlations, and there were no differences in the correlations that were significant at the p<.001 level (parametric correlations were therefore reported as these are used in the regression analyses). Cooks distances were calculated to examine the impact of outliers, and there were no significant outliers. Finally, all the other assumptions for regression were met; therefore it was considered that regression was appropriate.
Comparisons of thought control strategies between an adult sample (data extracted from Wells and Davies, Reference Wells and Davies1994) and the current adolescent sample are presented. As the adult data were reported by gender, the comparisons were also made by gender. Significance levels were set at .05/10 (.005) due to the number of t-tests performed. Correlations between OC interference, thought control strategies and meta-cognitive beliefs are then presented. It was expected from previous research that there would be significant associations between different subscales on the measures of thought control and meta-cognition (e.g. Matthews et al., Reference Matthews, Reynolds and Derisley2007; Reynolds and Wells, Reference Reynolds and Wells1999) and therefore regression analyses were performed to test which thought control strategies and meta-cognitive beliefs predicted unique variance in OC interference scores. Significance levels were set at .05/48 (.001) due to the number of correlations performed. Power calculations were performed for these analyses. For medium effect sizes, 80% power and the significance set at the level described above (correcting for number of analyses done), the required sample size was 107 for the regression analyses, 146 for the t-tests and 162 for the correlations.
Finally, the mediation analysis is presented. We were interested in whether there was overall mediation of the relationships between thought control strategies and OC interference by meta-cognitive factors, as well as exploring individual meta-cognitions. Mediation effects were therefore tested using a multiple mediation model with all relevant meta-cognitions entered simultaneously. This was performed using the Preacher and Hayes macro for SPSS (Reference Preacher and Hayes2008b). The indirect effect of the independent variables (IV) on the dependent variable (DV) through the mediators (M) was quantified as the products of the effects of the IV on Ms (a1, a2, a3), and the effect of Ms on the DV partialling out the effect of the IV (b1, b2, b3; see Figure 1). As recommended by Preacher and Hayes (Reference Preacher and Hayes2008a), a bootstrap approach was used with 5000 estimates of the indirect effect. This derives a point estimate of the indirect effect and 95 percentile-based confidence intervals. If these confidence intervals do not include 0, they are considered significant. As the CIs are estimated empirically using this method, they are not necessarily symmetrical.

Figure 1. Mediation of thought control strategies and OC interference by meta-cognitive beliefs.
Results
Comparisons between adolescent and adult thought control strategies
TCQ subscale scores were extracted from those reported in Wells and Davies (Reference Wells and Davies1994) of a non-clinical student sample aged 18–47 years and these scores were used to compare adolescent and adult data by gender (see Table 1). Adolescents reported using social control and reappraisal strategies significantly less frequently compared to an adult sample of participants, and adolescent males also reported using punishment less frequently than adult males. There was no significant difference in the reported use of distraction and worry strategies between the two samples. In both samples punishment and worry were the least used strategies and overall distraction was the most used strategy.
Table 1. A comparison of scores on thought control questionnaire between current sample of adolescents and an adult sample

a Data extracted directly from Wells and Davies (Reference Wells and Davies1994).
* p < .005.
Associations between thought control strategies, meta-cognitive beliefs and OCD symptoms
Correlations were performed using the two scores on the LOI-CV (OC symptoms and degree of interference) and both subscale and total scores on the TCQ and MCQ-A. This analysis was a little underpowered as the sample size recruited was 151, not 162 as required by the power calculation. Post-hoc power analysis suggested that the current study had a power of 76% to detect medium effect sizes. The significant correlations of OC symptoms and degree of interference with the other variables were identical and therefore results for OC interference scores only are presented (see Table 2). Significant positive correlations were found between OC interference and worry, punishment and reappraisal subscale scores, and the TCQ total score. A linear regression analysis was performed predicting OC interference from the five sub-scales of the TCQ (all entered in step one) and only worry and punishment predicted significant variance in OC interference scores (F (5, 145) = 8.02, p<.001, R2 = .22; worry t = 2.87, p<.001; punishment t = 2.11, p = .04; distraction t = −.45, p = .66; social control t = .34, p = .74; reappraisal t = 1.25, p = .21).
Table 2. Correlations between OC interference scores, thought control strategies and metacognitive beliefs
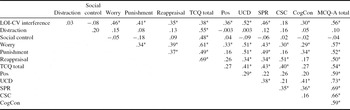
TCQ – thought control questionnaire; Pos – Positive beliefs about worry; UCD – Uncontrollability and danger beliefs; SPR – superstition, punishment and responsibility beliefs; CSC – Cognitive self-consciousness; CogCon – Cognitive confidence; MCQ-A – Metacognitions Questionnaire Adolescent version.
* p<.001.
N.B.: Correlations for LOI- CV total symptom score and TCQ and MCQ-A are available from the corresponding author.
Significant positive correlations were found between OC interference and positive beliefs, uncontrollability and danger beliefs, superstition, punishment and responsibility beliefs, cognitive confidence and the MCQ-A total score. The correlation between cognitive self-consciousness beliefs and obsessive-compulsive interference was not significant. A linear regression analysis was performed predicting OC interference from the five sub-scales of the MCQ-A (all entered at step one). Positive beliefs, uncontrollability and danger beliefs, and superstition, punishment and responsibility beliefs all predicted unique variance in OC interference scores (F (5, 145) = 13.64, p<.001, R2 = .32; PB t = 2.60, p = .01, UCD t = 4.29, p<.001, SPR t = 2.81, p<.006, CC t = .33, p = .74, CSC t = −.39, p = .70).
Mediation of relationships between thought control strategies and OC interference
In order to determine which mediation analyses were appropriate, thought control strategies were correlated with meta-cognitive beliefs (see Table 2). As worry and punishment uniquely predicted variance in OC interference scores, we focused on correlations with these two strategies. The strategy of worry was significantly correlated with all meta-cognitions, and punishment was significantly correlated with UCD, SPR and cognitive confidence beliefs. It was decided not to enter cognitive confidence or cognitive self-consciousness into the mediation analyses as they did not predict unique variance in OC interference scores. Therefore, one analysis examined whether UCD, SPR and positive beliefs mediated the relationship between worry and OC interference scores, and the second examined whether UCD and SPR beliefs mediated the relationship between punishment and OC interference scores (see Figure 1).
The summary of the mediation analyses is presented in Table 3. For both analyses the total effect (c) indicated significant relationships between worry/punishment, and OC interference scores. Each of the individual indirect effects (mediation effects of meta-cognitions) was also significant, and the 95% CIs did not include 0. The direct effects were not significant, indicating that meta-cognitive beliefs fully mediated the relationships between worry/punishment, and OC interference scores. There was evidence in support of all meta-cognitive mediators, so we conducted bias-corrected comparisons between the mediators. These indicated no significant contrasts. The mediation analyses suggest that UCD and SPR beliefs mediate the relationship between punishment and OC interference scores, and UCD, SPR and positive beliefs mediate the relationship between worry and OC interference scores.
Table 3. Summary of multiple mediator models for punishment and worry (n = 151; 5000 bootstraps)

* p<.05; ** p<.01.
Discussion
The current study aimed to explore thought control strategies and meta-cognitive beliefs in adolescence in order to examine whether the cognitive processes involved in adult OCD are relevant in a younger population. The results suggest that there are some similarities between the current sample of non-referred adolescents and previous samples of non-referred adults in these cognitive processes. In terms of thought control strategies non-referred adolescents and adults employ, punishment and worry are the least used strategies and distraction is the most used strategy (Wells and Davies, Reference Wells and Davies1994; see also Amir et al., Reference Amir, Cashman and Foa1997; Abramowitz, Whiteside, Kalsy and Tolin, Reference Abramowitz, Whiteside, Kalsy and Tolin2003; Coles and Heimberg, Reference Coles and Heimberg2005; Fehm and Hoyer, Reference Fehm and Hoyer2004; Morrison and Wells, Reference Morrison and Wells2000; Reynolds and Wells, Reference Reynolds and Wells1999; Roussis and Wells, Reference Roussis and Wells2006; Warda and Bryant, Reference Warda and Bryant1998). However, adolescents appear to use social control and reappraisal strategies significantly less frequently than published data using adult participants (for further data on adults see: Coles and Heimberg, Reference Coles and Heimberg2005; Fehm and Hoyer, Reference Fehm and Hoyer2004; Wells and Davies, Reference Wells and Davies1994). Furthermore, male adolescents in the current study used punishment less than male adults in the Wells and Davies study (Reference Wells and Davies1994). As very few studies that report TCQ mean scores report them by gender, this result requires replication. The strategies of worry and punishment have been associated with OC symptoms in adults (Amir et al., Reference Amir, Cashman and Foa1997), but it is more unusual for reappraisal to be associated. Given that reappraisal was also used less frequently by the adolescents in the current study it may be that the strategy of reappraisal is important developmentally; examining your own thoughts and trying to change them may be less normative in a younger population, and therefore a high level of this kind of strategy may be more associated with difficulties. However, reappraisal did not uniquely predict OC symptoms in the regression analysis, and therefore it may be reappraisal's association with other thought control strategies that is important.
In terms of meta-cognitive beliefs, both adolescents and adults report a variety of these beliefs and most of these beliefs are related to OC symptoms in non-clinical populations. In the current study CSC beliefs were not associated with OC symptoms, in common with other studies of non-referred young people (Sica, Steketee, Ghisi, Chiri and Franceschini, Reference Sica, Steketee, Ghisi, Chiri and Franceschini2007). Previous studies of meta-cognitive beliefs in young people have not used regression analyses to examine specific meta-cognitive predictors of OC symptoms, but in several studies of adults, positive beliefs and/or UCD beliefs have predicted OC symptoms (Cartwright-Hatton and Wells, Reference Cartwright-Hatton and Wells1997; Gwilliam, Wells and Cartwright-Hatton, Reference Gwilliam, Wells and Cartwright-Hatton2004; Sica et al., Reference Sica, Steketee, Ghisi, Chiri and Franceschini2007; Wells and Papageorgiou, Reference Wells and Papageorgiou1998). SPR beliefs have not previously been found to predict OC symptoms in adult participants and therefore this needs replication in order to determine whether this is a developmental difference. This is particularly important given the mediating role of SPR beliefs in the relationships between OC interference and the thought control strategies, worry and punishment. The two studies that have explored a mediating role for cognitions in the relationship between thought control strategies and OC symptoms in adult samples did not use the MCQ and therefore direct comparisons cannot be made. However, Moore and Abramowitz (Reference Moore and Abramowitz2007) found that obsessive beliefs, measured by the Obsessive Beliefs Questionnaire (OBQ; Steketee et al., Reference Steketee, Frost, Bhar, Bouvard, Calamari and Carmin2003), fully mediated the relationship between punishment and OC symptoms. Tolin et al. (Reference Tolin, Worhunsky, Brady and Maltby2007) found that only one thought control strategy, punishment, correlated with only one subscale of the OBQ, importance/control of thoughts, and that importance/control of thoughts fully mediated the relationship between punishment and OC symptoms. It is interesting therefore that cognitive factors as measured by the MCQ, fully mediated the relationship between OC interference scores and both worry and punishment strategies in the present non-referred adolescent sample. This may be interpreted as meaning that it is not only the individual cognitive factors in OC symptoms that are similar between adults and adolescents, but also the processes by which they work. However, this interpretation should be considered tentative, and should be directly tested.
It is important to examine the relevance of adult cognitive models to younger populations because although certain aspects of cognitive and emotional development are stable from about age 12, other aspects are not (Larson, Csikszentmihalyi and Graef, Reference Larson, Csikszentmihalyi and Graef1980; Rosenblum and Lewis, Reference Rosenblum, Lewis, Adams and Berzonsky2003). In particular, early adolescence is marked by increased sensitivity to social-emotional stimuli, with later adolescence being a time in which there is increased cognitive control and self-regulation (Casey et al., Reference Casey, Getz and Galvan2008). Perhaps it is only by later adolescence that cognitive and affective processes are effectively co-ordinated (Steinberg, Reference Steinberg2008), and therefore cognitive models of emotional disorders might be less relevant in this period of development. The limited evidence to date, supported by the findings of the current study, suggests that for OCD, cognitive-behavioural models of OCD may be applicable from adolescence (Cartwright-Hatton et al., Reference Cartwright-Hatton, Reynolds, Wilson, Silverman and Field2011; Reynolds and Reeves, Reference Reynolds and Reeves2008), and indeed therapies utilizing these models have been found to be effective in this population (Williams et al., Reference Williams, Salkovskis, Forrester, Turner, White and Allsopp2010). Validation of these models in adolescents may help in understanding and treating young people with OCD.
This study is a preliminary exploration of some cognitive factors associated with OCD symptoms in adolescence and has several limitations. The current study focused on a variety of meta-cognitive beliefs that have been found to be important in OCD. However, they have also been found to be important in other disorders and it may be that there are specific meta-cognitive factors involved in OCD, such as responsibility beliefs or thought-action fusion beliefs, that have not been measured in the current study. Furthermore the cross-sectional nature of the study does not allow any conclusions to be drawn about the role of these cognitive factors in the development or maintenance of OCD. Given that patterns of pre-treatment thought control strategies and changes in meta-cognition are associated with differential response to treatment (Reynolds and Wells, Reference Reynolds and Wells1999; Solem et al., Reference Solem, Håland, Vogel, Hansen and Wells2009), additional research is crucial to explore these factors in children and adolescents. The current study also involves a non-referred sample of adolescents, with a small, potentially biased, recruitment. Studies of adults with OCD show different patterns of thought control use compared with healthy controls, with distraction being used less frequently than reappraisal and punishment (Amir et al., Reference Amir, Cashman and Foa1997; Abramowitz et al., Reference Abramowitz, Whiteside, Kalsy and Tolin2003). Therefore studies of adolescents with OCD are required. Additional differences between Wells and Davies' adult participants and the participants in the current study, such as levels of depression or other psychological disorders, could also account for the differences in thought control strategies. Very few studies that report mean scores on the TCQ for non-clinical participants report demographic information for those participants, and those who do (for example, Fehm and Hoyer, Reference Fehm and Hoyer2004), do not analyze any differences. However, although most of the studies measure anxiety and depression, and indeed find significant associations between these variables and subscales of the TCQ, the two studies that control for anxiety and depression found that they did not change group differences (Abramowitz et al., Reference Abramowitz, Whiteside, Kalsy and Tolin2003; Reynolds and Wells, Reference Reynolds and Wells1999). It is possible, however, that both anxiety/depression and demographic factors can account for the differences found between adolescents in the current study, and studies of non-referred adults, and thus further research is required to confirm the current study's findings.
Despite these limitations, the current study finds that adolescents do use a variety of thought control strategies, and that these are associated with OC symptoms. Furthermore, meta-cognitions mediate the relationships between the strategies of worry and punishment and OC symptoms. Further research is required to determine whether there are robust gender differences in the development of thought control strategies, and whether thought control strategies and meta-cognitions are different in young people with OCD compared to young people with no psychological disorders, and young people with other anxiety disorders.





Comments
No Comments have been published for this article.