



Introduction
Cognitive behavioural therapy (CBT) is the most widely studied form of psychotherapy (Hofmann et al., Reference Hofmann, Asnaani, Vonk, Sawyer and Fang2012) and has been widely accepted by clinicians, researchers and service users as the first-line therapeutic approach for many child and adolescent mental health problems (Butler et al., Reference Butler, Chapman, Forman and Beck2006). This popularity has given rise to many clinicians using CBT methods resulting in clinicians presenting themselves as CBT practitioners even though they have not received sufficient training or acquired the necessary skills to deliver CBT competently. This results in the effectiveness of CBT being diluted and the expectations of service users not being met (Friedberg, Reference Friedberg2014). Becoming a competent CBT practitioner requires a vigorous training process involving both theoretical awareness, skills-based practice and supervision from experienced CBT trainers. Subsequently, this raises the question of how the competence of a CBT practitioner working with the child and adolescent population can be evaluated most objectively and based on what criteria.
In CBT, competence is defined as the degree to which the therapist demonstrates the general therapeutic and treatment-specific skills required to properly implement evidence-based CBT interventions (Muse and McManus, Reference Muse and McManus2013). Roth and Pilling (Reference Roth and Pilling2007) grouped a list of more than fifty ‘core competences’ needed to provide effective CBT in five key areas: general therapeutic competences (adequate knowledge in mental health and effective communication with the patient); general competencies related to CBT (ability to understand and explain CBT rationale); CBT specific competence (skills such as guided discovery, use of thought records); problem-specific competencies (awareness and ability to use problem-specific treatment manuals); and meta competencies (the capacity to choose and apply the most appropriate CBT method) (Roth and Pilling, Reference Roth and Pilling2007). A related concept is therapy fidelity or adherence. Adherence refers to the extent to which the therapist’s approach fits the model of therapy (Muse and McManus, Reference Muse and McManus2013), how faithful therapy is to the theory, and to what extent the therapy guidelines remain within the proposed frameworks. Several frameworks have been proposed that aim to draw attention to and thus close the gap between routine CBT practice in the clinical room and ideal CBT. The framework proposed by Roth and Pilling (Reference Roth and Pilling2008) offers a very comprehensive definition for CBT competence (Roth & Pilling, Reference Roth and Pilling2008). Miller (Reference Miller1990), on the other hand, offers a framework model for competence where clinical skills are assessed in four hierarchical categories: knowledge (knows), practical understanding (knows how), skills (shows how), and clinical practice (does) (Miller, Reference Miller1990). A successful CBT application should be evaluated by both how much adherence is provided to the cognitive model of therapy and how competently therapy techniques are applied (McGlinchey and Dobson, Reference McGlinchey and Dobson2003).
The two most commonly used and widely regarded as ‘gold standard’ measures for assessing CBT competence with adults (Muse and McManus, Reference Muse and McManus2013) are the Cognitive Therapy Scale (CTS; Young and Beck, Reference Young and Beck1980) and the Cognitive Therapy Scale-Revised (CTS-R; Blackburn et al., Reference Blackburn, James, Milne, Baker, Standart, Garland and Reichelt2001). Both scales evaluate the clinicians’ direct practice, have good psychometric properties, and are frequently used in CBT training settings. However, while these scales are valuable, they do not address competence issues specific to undertaking CBT with children and adolescents. They were developed for use with adults and do not reflect the developmental issues that arise when practising CBT with children and adolescents. This lack of developmental sensitivity has been questioned (Fuggle et al., Reference Fuggle, Dunsmuir and Curry2012). In particular, systemic influences in the onset and maintenance of the child’s problems need to be considered; appropriate adaptations to CBT should be made to reflect the child’s developing cognitive, emotional, linguistic and reasoning abilities; a richer creative ability and greater use of non-verbal methods are required to communicate abstract concepts in simpler, clearer and more understandable ways (Fuggle et al., Reference Fuggle, Dunsmuir and Curry2012; Stallard, Reference Stallard2020). This is consistent with others who found that the factor structure of the CTS differs depending on the clinical population it is used with (Affrunti and Creed, Reference Affrunti and Creed2019).
The Cognitive Behaviour Therapy Scale for Children and Young People (CBTS-CYP) (Stallard et al., Reference Stallard, Myles and Branson2014) was developed to provide an objective assessment of general CBT competence when working with children and adolescents. The aim was to develop a scale to assess the overall quality and adequacy of the CBT applied in the therapy session, rather than a detailed assessment of the way specific techniques such as exposure, behavioural experiments or guided discovery were conducted. The initial UK evaluation demonstrated that the CBTSCYP had good reliability and face validity, and matched well with the CTS-R in discriminative ability based on total score and single item criteria (Stallard et al., Reference Stallard, Myles and Branson2014). However, it would be valuable to investigate how valid and reliable the CBTS-CYP is in assessing CBT applied in different linguistic and cultural settings, and to conduct a comparative analysis with other CBT competence measuring tools more commonly used there.
Aim
There is increased interest in the development of CBT training in Turkey. There are two associations operating in Turkey in order to make CBT available to wider patient populations and thus to enable more mental health professionals to access CBT training. These associations are accredited by the European Association for Behavioral and Cognitive Therapies (EABCT) and offer training in accordance with EABCT and Academy of Cognitive Therapy (ACT) standards. However, CBT is a relatively new field of clinical practice in Turkey and the number of experienced and nationally/internationally accredited CBT trainers and supervisors in this field is low. This poses an even greater problem for professionals working with children and adolescents. Session recordings submitted for routine supervision or, in particular, for the purpose of accreditation are often made by assessors who do not have experience of working with children and adolescents, using CBT competence assessment scales that are not specific to this age group.
Therefore, the aim of the present study is to determine whether the CBTS-CYP is a valid and reliable tool for assessing CBT competence in the Turkish sample, in comparison with the CTS currently used in Turkey for this purpose. As a result, a CBT competence assessment tool more suitable for the paediatric age population will be made available to mental health professionals working in this field.
Method
Sample and procedure
The Cognitive Behaviour Therapy Scale for Children and Young People (CBTS-CYP) was used in a CBT supervision course that involved a total of 80 hours of supervision in 10 meetings via an online videoconferencing platform between July 2020 and February 2021. The training was organized by the Turkish Association of Cognitive Behavioural Psychotherapies (BDPD), which was established in 2011 with the aim of advancing CBT training in Turkey and one of two organizations accredited by the EABCT.
CBT supervision training for supervisees is attended by approximately 50 trainees who have passed the exam at the end of the 80-hour theoretical training. A week before the online supervision meeting, the trainee shares with all other trainees a preliminary information form that includes the case summary from a developmental perspective, case conceptualization, therapy goals and a summary of what has been done in the previous therapy sessions. The trainee also shares the audio or video recording of the session with the supervisor, provided that written consent is obtained from the patient. The recorded session is listened to/watched by the group and then scored by all participants, including the supervisor and the trainee themselves, through an electronic Google survey form containing the items in CTS and CBTS-CYP (CETPÖ). The result of this scoring – if the trainee approves – is shared with the whole group. Thus, the trainee will have the opportunity to compare his own score for his performance with the points given to his performance by the supervisor and the peer group. Afterwards, feedback is received from the trainee and other participants about the session and the therapy process. It is then concluded with the feedback from the supervisor and discussion about the strengths of the therapist and the aspects that need to be improved. If necessary, skill-building activities are carried out through role-play. The length of the shared sessions is usually around 40 minutes, and approximately four cases are supervised each training day. As there is no obligation to share cases in these supervisions, it is also a learning experience for those who are not ready to share their sessions in the supervision environment for various reasons. Preliminary information forms about shared cases provide a rich and practical resource for all participants with important information such as case summaries, problem formulation, therapy goals, exposure hierarchy, etc.
Data were collected from 51 different therapists attending the CBT supervision training who evaluated a total of 36 different clinical cases. The CTS was used by the rating therapists in the sessions together with the CBTS-CYP. Of the 51 therapists, one was an internationally accredited trainer and supervisor and five were experienced child and adolescent CBT therapists accredited by EABCT and ACT. The remaining therapists (n = 45) had at least 80 hours of formal CBT training and were practising CBT as one of the main therapeutic modalities in their daily clinical work. The supervisees were a group of mental health practitioners with different professional backgrounds and were practising in different working settings including a Tier-3 Child and Adolescent Mental Health Unit and private practice. They brought to the supervision the audio/video recordings of the cases they see in their daily practice to benefit from an environment of peer supervision and feedback from more experienced clinicians and accredited CBT trainers/supervisors. The choice of recorded sessions brought to the supervision were completely at the discretion of the supervisee. The client population consisted of children and young people aged between 7 and 18 years with mental health problems ranging from behavioural problems to cases with complex PTSD or severe OCD with co-morbid conditions. The majority of therapists were qualified child and adolescent psychiatrists (n = 28), and the remaining were psychologists (n = 10), psychological counsellors (n = 9), psychiatric nurses (n = 3) and a social worker (n = 1). The therapists were asked to listen to a full audio (sometimes video) recorded session and then to rate the session on a Google survey form containing both the CTS and CBTS-CYP. The sessions rated for the purpose of this study were between the 4th and 9th sessions of therapy.
The Cognitive Behaviour Therapy Scale for Children and Young People (CBTS-CYP)
The CBTS-CYP was based upon the CTS-R, which is a widely used assessment tool that provides a comprehensive overview of the generic and CBT specific skills required to competently practise CBT with adults (Fairburn and Cooper, Reference Fairburn and Cooper2011). CBTS-CYP contains all items included in the CTS-R; however, these items were modified where needed and items added to appropriately reflect the use of CBT with children and young people. Similar to the CTS-R, a 7-point Likert scale was adopted for use in the CBTS-CYP and the same thresholds for assessing competency, i.e. a minimum score of 2 on each item and at least 50% on the total score, were preserved (Stallard, Reference Stallard2020). As the CBTS-CYP includes items to evaluate both verbal and non-verbal behaviours, similar to the CTS-R, it can be used to assess both audio and video recordings of clinical sessions.
The item home assignments were initially subsumed within the discovery competence. The first version of the CBTS-CYP, therefore, consisted of 14 items. However, this item was then separated and identified as a discrete competency, like the CTS-R, in its current iteration.
The latest version of the CBTS-CYP contains a total of 15 items; the first seven assess process defined by the acronym PRECISE, and the remaining eight items assess methods defined by ABCDEFGH. The acronym PRECISE stands for the initial letters of the following items: Partnership based on collaborative empiricism; Right developmental level consistent with the young person’s cognitive, linguistic, memory and perspective taking abilities; Empathic warm, caring and respectful relationship; Creatively and flexibly conveying CBT concepts; Investigation and self-discovery; Self-efficacy built upon the strengths, skills and ideas of the young people; Enjoyable and engaging session. ABCDEFGH is referred to as the A, B, Cs of CBT and stands for the initial letters of the following items: Assessment that includes establishing clear goals and appropriate use of diaries, questionnaires, and rating scales; Behavioural techniques such as graded exposure, behavioural activation and activity scheduling; Cognitive techniques to identify cognitions, promoting cognitive awareness, challenge, reframe or to develop mindfulness, acceptance and compassion; Discovery facilitated by techniques such as the Socratic dialogue, behavioural experiments and prediction testing; Emotional techniques to identify and manage strong, unpleasant emotions; Formulation which highlights the relationships between events, cognitions, emotions, physiological responses and behaviour; General skills to effectively manage sessions such as agenda setting, session planning and managing challenging behaviour; Home assignments with clear goals and purpose. Each item is rated on a 7-point Likert scale (scored 0–6) assessing degree of competence giving a total score of 90.
The Cognitive Therapy Rating Scale (CTS)
Developed by Young and Beck (Reference Young and Beck1980), the CTS is a widely used observer-rated measure of CBT treatment fidelity (Goldberg et al., Reference Goldberg, Baldwin, Merced, Caperton, Imel, Atkins and Creed2020). It was originally developed to contain two theorized factors in 11 items: ‘general therapeutic skills’, which consist of six items (Agenda, Feedback, Understanding/Empathic skills, Interpersonal effectiveness, Collaboration, Pacing/use of time) and ‘cognitive-behavioural skills’ consisting of five items (Guided discovery/Empiricism, Focusing on key cognitions or behaviours, Strategy for change/conceptualization, Application of Cognitive behavioural techniques, and Homework). Each item is rated on a 7-point Likert scale (scored 0–6) to reflect the degree of competence giving a total score of 66. The CTS is the most commonly used scale for measuring CBT competence and fidelity, in training programs, clinical trials, for formal certification and in studies assessing effective CBT delivery (Affrunti and Creed, Reference Affrunti and Creed2019).
The CTS-R (Blackburn et al., Reference Blackburn, James, Milne, Baker, Standart, Garland and Reichelt2001) was designed as a revision of the CTS to improve its psychometric properties. The CTS-R presented coding on a scale in which the therapist’s attitudes were evaluated in a range between 0 (which is considered inadequate) and 6 points (which corresponds to excellent performance). The original CTS had a similar 7-point Likert scoring, but only explanations were provided for items corresponding to 0, 2, 4 and 6 points. As the three in-between response options were not defined, the CTS-R filled this gap and provided a consistent grading pattern for all items. In addition, the evaluation of ‘focusing on key behaviours and cognitions’, which is evaluated over a single item in CTS, is divided into ‘eliciting behaviours’ and ‘eliciting cognitions’. The expression ‘Elicitation of appropriate emotional expression’ has also been added to evaluate emotional processing as an independent item.
A study in which the CTS and its revision, the CTS-R, were used comparatively in a sample with depression, showed that both CTS and CTS-R gave similar results in terms of internal reliability and inter-rater reliability. It has been reported that both can predict a significant decrease in depression symptoms at the end of therapy (Kazantzis et al., Reference Kazantzis, Clayton, Cronin, Farchione, Limburg and Dobson2018).
Translation of the CBTS-CYP into Turkish
Firstly, the translation of the scale from English to Turkish was made by an independent expert in the field of child and adolescent psychiatry and then evaluated by the research team. The Turkish translation of the scale was then back-translated into English by a professional translator, who had no specific expertise in the field of mental health. The back-translated scale was examined by a bilingual English-speaking researcher with expertise in CBT for its integrity and appropriateness. The scale was piloted, suggestions about the comprehensibility of the items obtained and the final version of the translation was approved by the team. The main issue with the translation was about how to preserve the PRECISE and ABCDEFGH acronyms. As we could not come up with Turkish equivalents of these acronyms, we decided to use them as they were and encouraged the therapists to memorize them before the theoretical CBT training commenced. We then provided a brief re-training for both CTS and CBTS-CYP at the beginning of supervision meetings.
Data evaluation and analysis
The data obtained were statistically analysed using the SPSS 24.0 (Statistical Package of Social Science) package programme. Parallel form correlations for equivalence, inter-rater reliability for stability, and Cronbach’s alpha value for internal consistency/homogeneity were conducted for reliability analysis. Finally, language validity and construct validity analyses were made.
Results
Descriptive statistics
The ages of 36 clients, whose cases were presented for supervision were between 8 and 18 years of age (14.10 ± 2.54). Six (17%) of the cases were male and 30 (83%) were female. The primary diagnoses of the presented cases were depression (5), obsessive-compulsive disorder (13), social anxiety disorder (5), generalized anxiety disorder (4), specific phobia (4), post-traumatic stress disorder (2), eating disorder (1), agoraphobia (1) and separation anxiety disorder (1).
Inter-rater reliability
For each case (n = 36), a number of therapists ranging from 32 to 51 evaluated the audio or video recording. Thus, the inter-rater reliability of the CBTS-CYP for each interview was obtained with the intraclass correlation coefficient (ICC) values. According to Shrout and Fleiss (Reference Shrout and Fleiss1979), in the case of several raters assessing the same target, a two-way mixed effects approach ICC with absolute agreement would be an appropriate approach (Shrout and Fleiss, Reference Shrout and Fleiss1979). The results showed that the ICCs ranged between 0.698 and 0.968 for the process items; 0.702–0.947 for the method items; and between 0.994 and 1.000 for the total form. Thus, the results demonstrated that the intraclass correlation values were good (0.60–0.74) or excellent (0.74 and above). Table 1 shows the ICC values of five interviews randomly selected from 36 sessions through the analysis program.
Table 1. Intraclass correlation values for a sample of sessions

Examination of correlations between CBTS-CYP and CTS
For all evaluations, correlations between CBTS-CYP total and subscale scores and CTS total scores were examined. Pearson’s correlation coefficient between the CBTS-CYP and CTS total scores was 0.935 (p < 0.001). Correlation coefficients between the CBTS-CYP process and method sub-dimensions and the CTS total score were respectively 0.889 and 0.921 (p < 0.001). In addition, the correlations of each CBTS-CYP item and CTS items were examined, and all relationships were found to be significant. Table 2 presents the results.
Table 2. Correlations between CBTS-CYP and equivalent CTS items

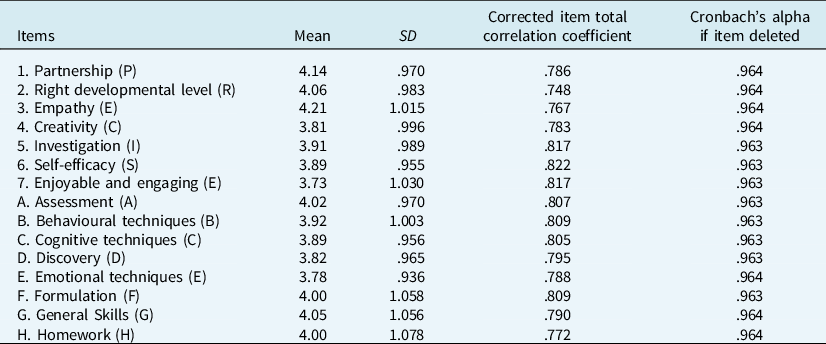
Item analysis and internal consistency analysis
Item analysis was used to evaluate the quality and distinctiveness of the scale items. Item-total correlation values corrected according to item analysis results ranged from .748 to .822 (Table 3). The internal consistency of the scale was tested using the Cronbach alpha value. The total-scale Cronbach alpha value was found to be .94. The Cronbach alpha value for the process sub-dimension was .93, and for the method sub-dimension was .94.
Table 3. Item analysis results
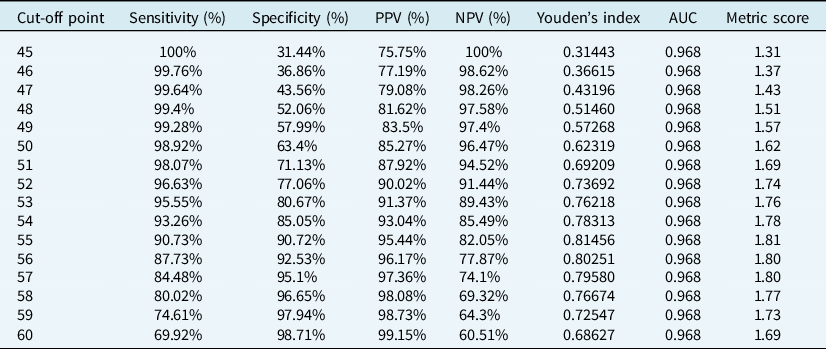
Sensitivity, specificity, positive predictive value, negative predictive value and cut-off point
The CTS cut-off score of 40 or more points was used to determine the cut-off score of CBTSCYP. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and cut-off point for CBTS-CYP were calculated using the ROC curve. ROC analysis results under the curve were found to be significant with a value of .968. The value where the sensitivity and specificity values were closest to each other and to 100% was chosen as the place where the cut-off score was determined. The cut-off point obtained when the sensitivity reached 90.73% and specificity 90.73% was found to be 55. In this context, considering that the total score of CBTS-CYP is 90, the specificity value drops to 31.44%, when the cut-off is taken as 45. The results are shown in Table 4. The ROC curve is as given in Fig. 1.

Figure 1 ROC curve for CBTS-CYP.
Table 4. CBTS-CYP total ROC analysis
Discriminative ability
Ratings provided by each rater based on both CBTS-CYP and CTS are shown comparatively in the supplementary table. For both rating scales, a score of 2 or less on any item or receiving less than a total score of 40 points for the CTS and 55 points for the CBTS-CYP was considered a ‘failure’. Findings are displayed in the Supplementary material.
Using the total score criteria, 17 recordings met the failure criteria; 15 (scored less than 55) on the CBTS-CYP and 15 (less than 40) on the CTS. Of these, 13/17 (76%) were identified by both the CTS and the CBTS-CYP. Using the single item criteria (score less than 2), 12 recordings were failed, with 11 (92%) being identified by both measures. Of the 18 cases who failed on either criterion, 16 (89%) were identified by both the CBTS-CYP and CTS
Discussion
This is the first study to examine the psychometric properties of the CBTS-CYP as a child and adolescent CBT-oriented competence and fidelity assessment tool in the Turkish language, and the first reliability and factor structure analysis of the CBTS-CYP in a different setting and culture. The results presented here are consistent with the previous study (Stallard et al., Reference Stallard, Myles and Branson2014) and show that the CBTS-CYP (its translation into Turkish is abbreviated as ÇETPÖ) has high levels of inter-rater reliability and correlations with the well-established CTS (Affrunti and Creed, Reference Affrunti and Creed2019; Borkovec et al., Reference Borkovec, Newman, Pincus and Lytle2002; Young and Beck, Reference Young and Beck1980). It has good discriminative ability that is comparable with the CTS. Finally, it has good acceptability with the raters liking the scale and feeling it was comprehensive and easy to use with limited training.
Determining the criteria for demonstrating competence is complex and will continue to be debated. It is further compounded by inconsistent scorings among different assessors (James et al., Reference James, Blackburn and Reichelt2001; Keen and Freeston, Reference Keen and Freeston2008; Stallard et al., Reference Stallard, Myles and Branson2014). The usual dual criteria used for demonstrating competence on the CTR and the CTS-R are a minimum total score and single item thresholds. Our findings demonstrate that when the CBTS-CYP cut-off score of 55 was adopted (equivalent to 40/66 on the CTS), the sensitivity of the total scale was 90% and the specificity was 90%. In terms of pass criteria, both scales identified 13/17 (76%) who failed the total score criteria, 11/12 (92%) who failed the single item criteria and 16/18 (89%) who failed either criterion.
The optimal CBTS-CYP cut-off of 55 found in this study is higher than that previously reported (i.e. 42) when compared against the CTS-R. Whilst this paper has evaluated the updated version of the CBTS-CYP with one additional item, the overall criteria to determine competence by the CTS-R and CTS differ. The CTS-R requires a total score equivalent to 50% or more (i.e. 36/72) whilst the CTS requires a score of 60% or more (i.e. 40/66). Although the total score cut-offs of the CBTS-CYP are consistent with those recommended by the comparison scales, it nonetheless raises the question of what level is required to demonstrate competence. In this study, three recordings met the total score pass criteria but failed on one or more single item. Given that the aim of the CBTS-CYP is to assess competence across the range of skills required to undertake CBT with children and young people, the use of a dual criteria approach appears justified.
Although these rating scales are often used to evaluate a single session, especially when used for accreditation of the therapist by an institution, it could be problematic to assess multi-dimensional constructs such as competence and adherence in a single session recording. For example, a single session may not be sufficient to evaluate whether a range of cognitive and behavioural techniques including interventions such as behaviour experiments and exposure were used correctly at the right time.
From this point of view, it may be useful to determine more clearly the application areas where these scales would provide a healthier evaluation. In addition to evaluating a single session recording, written material including additional information about the therapy process, case summary, case conceptualization, therapy goals, techniques used in sessions other than the current session, therapy planning, etc. should also be included in the competence assessment. These scales should be the tool of a process in which competence assessment is done on cross-sectional as well as dimensional planes.
The P in CETPÖ, the Turkish equivalent of CBTS-CYP, represents the first letter of the word ‘performance’ (performance is translated into Turkish as ‘Performans’). It is also debatable whether what these scales really assess is the performance demonstrated in the cross-sectional assessment of a single session, or the therapist’s competence as a CBT therapist more generally. Of course, if competence refers to a dimensional and longitudinal rather than cross-sectional assessment, the minimum criterion to be considered competent must be something more than exceeding a cut-off score from these scales. Roth and Pilling (Reference Roth and Pilling2008) report that the rather comprehensive framework they have drawn up with an evidence-based methodology cannot be used in its current form for a systematic assessment of CBT competences (Roth and Pilling, Reference Roth and Pilling2008). On the other hand, the same authors suggested that the 25-item Cognitive Therapy Adjustment and Competence Scale (CTACS; Barber et al., Reference Barber, Liese and Abrams2003) and the 14-item CTS-R (Blackburn et al., Reference Blackburn, James, Milne, Baker, Standart, Garland and Reichelt2001) that only include subsets of items proposed in their detailed and voluminous framework could effectively and reliably deliver an assessment of competence. Similarly, for the purpose of assessing the CBT therapist competence, Muse and McManus (Reference Muse and McManus2013) placed the measures that rate actual therapy sessions at the highest level of clinical skills hierarchy.
Another important question to be answered is whether CBTS-CYP (CETPÖ) and CTS (or CTS-R) really measure the same competences. The study of Stallard et al. (Reference Stallard, Myles and Branson2014), in which the CBTS-CYP scale was developed, showed that some items in CBTS-CYP do not have a direct equivalent in CTS-R. Items such as Right developmental level (R), Creativity (C), Self-efficacy (S) and Enjoyable and engaging (E) included in the PRECISE acronym, which represents the ‘process’ items of the CBTS-CYP framework, have no direct counterparts in the CTS-R. Similarly, Assessment and goals (A) in the ABCDEFGH formula, which represents the ‘Method’ items of the CBTS-CYP framework, does not have a direct equivalent in CTS or CTS-R. However, all competence items in the CTS-R or CTS are also available in CBTS-CYP, and the correlations between the two scales were found to be high on the basis of both the item-level and the total scale score. Beyond these statistical data, when CBTS-CYP is used to measure the competence of therapy with children and adolescents, it not only covers all areas evaluated by CTS, but also adds depth by providing an evaluation from a developmental perspective.
On another note, in competence assessments made by listening to audio recordings, it should be taken into account that there may be potential difficulties with the full assessment of some of the competence items. For example, the criterion of ‘appropriately responding to the child’s and carers’ verbal and non-verbal expressions and emotional responses such as distress, excitement or anxiety’ suggested in the CBTS-CYP for the evaluation of ‘Empathy’ may not be scored ideally. Similarly, it may not be observed how the therapist uses a range of non-verbal techniques for the assessment of ‘Creativity’.
Whilst this study highlights the robustness of the CBTS-CYP to assess competence in undertaking CBT with children and adolescents in Turkey, it does have a number of limitations. Firstly, the number of evaluators (n = 32–51) and recordings assessed (n = 36) are relatively small. Secondly, the evaluation was undertaken within one implementation program and as such further studies are required to investigate whether these findings generalize to other settings. Thirdly, although recordings included children aged 8–18 years, the majority were teenagers with few under the age of 11. The use of CBT with younger children requires more creativity, family involvement and adaptation to ensure that it is developmentally appropriate. The appropriateness of the CBTS-CYP to assess CBT with this younger age group needs to be determined.
In conclusion, this study has added to the literature regarding the psychometric robustness of the CBTS-CYP to assess competence in undertaking CBT with children and young people. The CBTS-CYP is comparable to established ‘gold standard’ measures widely used to assess competence with adults. Importantly, the Turkish translation of the CBTS-CYP provides a useful tool for evaluating competence where child and adolescent expertise is limited.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1352465822000169
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article and/or its supplementary materials.
Acknowledgements
None.
Author contributions
Vahdet Gormez: Conceptualization (lead), Data curation (equal), Formal analysis (supporting), Investigation (equal), Methodology (equal), Project administration (equal), Writing – original draft (lead), Writing – review & editing (lead); Süleyman Çakıroğlu: Data curation (equal), Formal analysis (equal), Methodology (equal), Software (equal); Alperen Bıkmazer: Data curation (equal), Formal analysis (equal), Methodology (equal), Project administration (equal); Paul Stallard: Conceptualization (supporting), Data curation (supporting), Methodology (equal), Validation (equal), Writing – original draft (supporting), Writing – review & editing (supporting).
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of interest
The authors declare none.
Ethical standards
The authors confirm that they have abided by the Ethical Principles of Psychologists and Code of Conduct as set out by the BABCP and BPS. The study was approved by the Istanbul Medeniyet University Ethics Committee.








Comments
No Comments have been published for this article.