


Introduction
Paranoia has been defined as “a disordered mode of thought that is dominated by an intense, irrational, but persistent mistrust or suspicion of people and a corresponding tendency to interpret the actions of others as deliberately threatening or demeaning” (Fenigstein, Reference Fenigstein and Friedman1994). More recently, Freeman and Garety (Reference Freeman and Garety2000) have defined paranoia as the belief that harm is occurring or is going to occur, and that the persecutor has the intention to cause harm to the person. Paranoia occurs across a wide range of psychopathologies, such as depression, social phobia, personality disorder and psychosis (American Psychiatric Association, 1994). However, far from being a disordered mode of thought, it is now acknowledged that paranoia is a common experience, which is by no means unique to clinical populations. In his review of paranoid thinking in non-clinical populations, Freeman (Reference Freeman2007) reported a conservative estimate that 10–15% of the general population regularly experience paranoid thoughts. Some of the variance in findings across these studies can be accounted for by how paranoid thoughts are measured. Specifically, more fleeting and transient paranoid thoughts are unlikely to be recorded in epidemiological studies that use formal diagnostic interview schedules (e.g. Tien and Anthony, Reference Tien and Anthony1990) in contrast to studies that allow for a wider definition of paranoid thinking (e.g. Johns et al., Reference Johns, Cannon, Singleton, Murray, Farrell, Brugha, Bebbington, Jenkins and Meltzer2004; Freeman et al., Reference Freeman, Garety, Bebbington, Smith, Rollinson, Fowler, Kuipers, Katarzyna and Dunn2005a). Furthermore, Freeman et al. (Reference Freeman, Garety, Bebbington, Smith, Rollinson, Fowler, Kuipers, Katarzyna and Dunn2005a) found evidence for a hierarchical structure to paranoid thinking, beginning with relatively common social evaluative concerns; having ideas of reference (e.g. that people are talking about you); mildly threatening thoughts (e.g. that people are trying to cause some minor distress); moderately threatening thoughts (e.g. that people are going out of their way to get at you) and severely threatening thoughts (e.g. people are trying to cause serious harm and are involved in conspiracies against you). The weekly occurrence of social evaluative concerns was observed in 30–40% of respondents, compared to the weekly occurrence of seriously threatening paranoid thoughts in 5%. This hierarchical model of paranoia can be contrasted with previous understandings of paranoia. For example, Fenigstein and Vanable (Reference Fenigstein and Vanable1992) defined sub-clinical paranoia as a style of thought manifested by exaggerated self-referential biases that arise in ordinary, daily behaviour. Importantly, this mode of thought was conceptualized as a relatively consistent bias toward suspiciousness, feelings of resentment and ill will, mistrust, and a belief in external control. Freeman's hierarchical organization of paranoia is interesting because it allows researchers and clinicians to raise questions of what additional factors might contribute to increasing frequency and distress associated with the ebb and flow of paranoid thinking. In particular, given that paranoid thoughts are normally occurring and spontaneous appraisals related to the perceptions of interpersonal threat and danger, it is of interest to investigate what factors may be associated with the increased availability of such specific threat related appraisals. Candidate variables that are likely to relate to processes including increased self-consciousness (e.g. Fenigstein, Reference Fenigstein1984), the presence of negative affect and emotional distress (e.g. Freeman, Reference Freeman2007), the tendency to worry (thus increasing the general availability of a stream of threat related cognitions) (e.g. Morrison and Wells, Reference Morrison and Wells2007) and, finally, the beliefs a person has about paranoia as a helpful strategy, or the extent to which they may fear and thus become vigilant for and have a ruminative focus on paranoid thoughts (Morrison et al., Reference Morrison, Gumley, Schwannauer, Campbell, Gleeson, Griffin and Gillan2005).
Self-consciousness
Given the close association between paranoid thinking and social evaluative concerns, one potential factor that may account for increased paranoid thinking is self-consciousness. Fenigstein and his colleagues have also emphasized the relationship between self-consciousness and “paranoia” where paranoia emerges from a tendency to over perceive oneself as a target (the self-as-target bias) (Fenigstein, Reference Fenigstein1984; Fenigstein and Vanable, Reference Fenigstein and Vanable1992). Self-focus also plays a central role in self-regulation, and many disorders result from the inappropriate application of self-regulatory strategies (Carver and Scheier, Reference Carver and Scheier1981). In addition, there is support for the theory that self-focus may operate to activate or increase the availability of self-referent cognitions and thus influence the emergence of threat appraisals. In a study of 30 individuals with psychosis, Smari, Stefansson and Thorgilsson (Reference Smari, Stefansson and Thorgilsson1994) found that paranoia was associated with increased self-consciousness and social anxiety. Morrison and Wells (Reference Morrison and Wells2007) found that delusional distress was predicted by social worry having controlled for severity of delusional beliefs. The particular finding that social worry was predictive of delusional distress is consistent with the suggestion that there are clear similarities and overlapping processes between social anxiety processes, including self-consciousness and persecutory ideation, and the conceptualization of paranoia as a preoccupation with interpersonal threat (Fenigstein and Vanable, Reference Fenigstein and Vanable1992; Freeman and Garety, Reference Freeman and Garety2000).
Negative affectivity
Freeman and Garety (Reference Freeman and Garety2003) have previously noted the close correspondence between the content of persecutory beliefs and the accompanying emotions, for example depression associated with persecutory beliefs about punishment, or anxiety associated with the perception of other people talking behind a person's back. Freeman (Reference Freeman2007) has shown that the relationship between persecutory beliefs and anxiety has been repeatedly reported. Paranoid thoughts build upon common interpersonal anxieties and anxiety has been found to be predictive of the occurrence of paranoid thoughts (Freeman et al., Reference Freeman, Slater, Bebbington, Garety, Kuipers, Fowler, Met, Read, Jordan and Vinayagamoorthy2003, Reference Freeman, Garety, Bebbington, Slater, Kuipers, Fowler, Green, Jordan, Ray and Dunn2005b). There is also evidence that increased depression is associated with more frequent paranoid thoughts. Green et al. (Reference Green, Freeman, Kuipers, Bebbington, Fowler, Dunn, and Garety2008) found moderate associations between the Paranoid Thoughts Scale and both anxiety and depression (r = 0.39 and 0.50 respectively). Freeman, Pugh, Vorontsova and Southgate (Reference Freeman, Pugh, Vorontsova and Southgate2009) found that depression and anxiety were associated with an increased odds of experiencing paranoid thoughts (OR = 1.31 and 2.12 respectively).
Worry
Related to anxiety, worry is also a common problem in paranoia. It may be that an increased tendency to worry, as evidenced by more negative interpretations of general worry related thoughts, is linked to greater availability of paranoia related thoughts, especially since paranoid thoughts like worry are threat related appraisals. Similar processes responsible for the vulnerability to and maintenance of worrying in GAD have also been suggested as being responsible for the maintenance of delusional distress. Using a clinical sample, Freeman and Garety (Reference Freeman and Garety1999) found that, as with distress about worry seen in GAD, delusional distress was not simply related to the content of thoughts. They found that meta-worry predicted the use of punishment thought control strategies in both persecutory delusions and anxiety groups. Patients experiencing delusional beliefs have been found to use more punishment and worry and less distraction thought control strategies compared to non-patients (Morrison and Wells, Reference Morrison and Wells2000). In addition, the tendency to catastrophize worry related thoughts is associated with the occurrence of non-clinical paranoia and with the maintenance of persecutory delusions (Startup, Freeman and Garety, Reference Startup, Freeman and Garety2007). Worry is also given an important role in cognitive models of paranoia (Freeman, Reference Freeman2007). Indeed, in a study of 24 individuals with persistent persecutory delusions, Foster, Startup, Potts and Freeman (Reference Foster, Startup, Potts and Freeman2010) found that targeting worry in a brief cognitive behavioural intervention was associated with reductions in worry and in delusional distress. Importantly, change in worry over 2 months was modestly associated with measures of change in paranoia (Range r(tau) = 0.34 – 0.49).
Beliefs about paranoia
Morrison et al. (Reference Morrison, Gumley, Schwannauer, Campbell, Gleeson, Griffin and Gillan2005) investigated the factor structure of the Beliefs about Paranoia Scale (BaPS) and whether individuals' beliefs about paranoia were predictive of their experience of paranoia and its associated distress in a sample of 317 non-patients. They identified a 4-factor structure measuring Negative Beliefs about Paranoia (e.g. my paranoia gets out of control), Paranoia as a Survival Strategy (e.g. it is safer to be paranoid), General Positive Beliefs (e.g. paranoia can make life seem more exciting and exhilarating) and Normalizing Beliefs (e.g. being paranoid is just human nature). Using multiple regression, negative beliefs and survival beliefs were associated with more frequent paranoid thoughts as measured by the Paranoia Scale (Fenigstein and Vanable, Reference Fenigstein and Vanable1992). In contrast, only negative beliefs were associated with distress associated with delusional ideation as measured by the Peters Delusions Inventory (Peters, Joseph and Garety, Reference Peters, Joseph and Garety1999). The finding that both negative and survival beliefs were associated with more frequent paranoid thoughts is consistent with a metacognitive conceptualization of paranoia. Paranoia may be employed as a deliberate strategy for managing interpersonal threat, similar to the use of worry for dealing with more general threats. The occurrence of negative beliefs about paranoia was uniquely associated with delusional distress, suggesting that negative beliefs may be particularly linked to distress arising from paranoia. However, several limitations to the BaPS were noted. The overall structure of the scale was unbalanced in that Positive Beliefs and Normalizing Beliefs had a small number of items (n = 4 and 3 respectively). In addition, the poor internal consistency of these factors (Positive Beliefs = 0.49; Normalizing Beliefs = 0.60) reflected a need to further develop these factors in order to create a balanced measure of beliefs about paranoia. Therefore this study aimed to investigate the role of beliefs about paranoia as predictors of frequency and distress of paranoia in a non-clinical population. Specifically, this study aimed to (a) revise and strengthen the Beliefs about Paranoia Scale (BaPS) for initial use in a non-clinical population by confirming the factor structure of the BaPS using confirmatory factor analysis (CFA) (EQS, Bentler, Reference Bentler1995). It was proposed that there would be a 4-factor solution consisting of Negative Beliefs about Paranoia, Paranoia as a Survival Strategy, General Positive Beliefs, and Normalizing Beliefs.
We hypothesized that survival beliefs about paranoia would be positively associated with frequency of paranoia and that negative beliefs about paranoia would be positively associated with distress about paranoia. We also hypothesized that the use of problematic thought control strategies (specifically punishment and worry) would be associated with frequency of paranoia. In testing these hypotheses, we also wished to control for self-consciousness and levels of anxiety and depression as these factors have been shown to be associated with greater paranoia.
Method
Participants and procedure
This study used a cross-sectional design with a sample of first year through to fourth year undergraduate students attending three higher education institutions. No financial or educational incentive was offered.
Measures
The Paranoia Scale (PS; Fenigstein and Vanable, Reference Fenigstein and Vanable1992) is a 20-item self-report questionnaire developed to assess frequency of sub clinical levels of paranoia. It is scored on a 1–5 likert scale with scores ranging from 20–100. The PS was the main dependent variable for all analyses. Higher scores reflect higher levels of sub clinical paranoia. The scale has demonstrated good internal consistency (alpha = 0.84) and stability (r = 0.70). For the purposes of this study the Paranoia Scale was modified to consist of an additional scale to measure distress for each item measured on a 1–5 likert scale. Internal consistency of the frequency scale and the distress scale for the current study was good (Cronbach's alpha = 0.91; 95% CI = 0.88 – 0.92 and alpha = 0.91; 95% CI = 0.87 – 0.92).
The Self-consciousness Scale (SCS; Fenigstein, Scheier and Buss, Reference Fenigstein, Scheier and Buss1975) measures self- consciousness dimensions, termed Private and Public Self-consciousness and Social Anxiety. Fenigstein et al. (Reference Fenigstein, Scheier and Buss1975) obtained high reliability coefficients for private self-consciousness (alpha = 0.79) and public self-consciousness (alpha = 0.84). Internal consistency for the current study was good (public: alpha = 0.87; 95% CI = 0.84 – 0.90, private: alpha = 0.70; 95% CI = 0.63 – 0.76, social anxiety: alpha = 0.79; 95% CI = 0.75 – 0.84).
The Hospital Anxiety and Depression Scale (HADS; Zigmond and Snaith, Reference Zigmond and Snaith1983) consists of 14 items and asks respondents to rate responses from a range of 0–3. The HADS was used to measure levels of anxiety and depression. Internal consistency for the anxiety scale ranged from alpha = 0.76 to 0 .41 and the depression scale ranged from alpha = 0.60 to 0.30. Internal consistency for the current study was good (anxiety: alpha = 0.88; 95% CI = 0.85 – 0.90) depression: alpha = 0.71; 95% CI = 0.64 – 0.77).
Thought Control Questionnaire (TCQ; Wells and Davies, Reference Wells and Davies1994) is a 30-item self-report questionnaire that assesses the effectiveness of strategies used for the control of unpleasant and unwanted thoughts. This measure asks about thoughts in general and is not specific to paranoid thoughts. Items are scored on a 4-point likert scale. It measures five factors that agree with different strategies for controlling unwanted thoughts and has good internal consistency (distraction: alpha = 0.72; social control: alpha = 0.79; punishment: = 0.64; worry: alpha = 0.64; and reappraisal: alpha = 0.67). Internal consistency was for the current study ranged from poor to good (distraction: alpha = 0.73; 95% CI = 0.67 – 0.79, social control: alpha = 0.30; 95% CI = 0.14 – 0.45, punishment: = 0.56; 95% CI = 0.45 – 0.65, worry: alpha = 0.83; 95% CI = 0.79 – 0.86 and reappraisal: alpha = 0.72; 95% CI = 0.65 – 0.78).
The Beliefs about Paranoia Scale (BaPS; Morrison et al., Reference Morrison, Gumley, Schwannauer, Campbell, Gleeson, Griffin and Gillan2005) is a self-report questionnaire developed to measure metacognitive processes involved in paranoia by measuring positive and negative beliefs about paranoia. It consists of a number of attitudes and thoughts that people have expressed about paranoia based on clinical knowledge of patients experiencing persecutory delusions. Items on the questionnaire were generated to measure hypothesized latent variable structures of negative beliefs about paranoia, positive beliefs about paranoia as an interesting way of thinking, as a survival strategy, and normalizing beliefs. A 50-item questionnaire was developed following preliminary validation of the 31-item version of the questionnaire in a previous study (Morrison et al., Reference Morrison, Gumley, Schwannauer, Campbell, Gleeson, Griffin and Gillan2005) using confirmatory factor analysis that suggested a 4-factor model of the BaPS, and that further scale development was desirable as the General Positive Beliefs and Normalizing Beliefs only had 4 and 3 items respectively. The scoring of the version used in this study was the same as Morrison et al. (Reference Morrison, Gumley, Schwannauer, Campbell, Gleeson, Griffin and Gillan2005).
Data analyses
Data were analysed using SPSS for Windows Version 11.5, and the structural equation modelling package EQS, Version 6.1 for Windows (Bentler, Reference Bentler1995) was used to test the goodness of fit of the BaPS to a 4-factor solution. Prior to formal factor analyses, the inter-item correlation matrix was examined to see if there was a predominance of correlations above 0.3 among the items supporting the suitability for factoring as recommended by Kline (Reference Kline1994). The adequacy of competing models of the BaPS was assessed through an examination of a variety of fit indices. Overall and incremental model fit was examined by model chi-squared (χ2) and the Comparative Fit Index (CFI: Bentler, Reference Bentler1995). A significant χ2 suggests that the data depart significantly from the model. A CFI <0.90 indicates that the model is an inadequate description of the data, whereas a model with CFI > 0.95 is regarded as fitting the data well (Bentler and Bonnet, Reference Bentler and Bonett1980). The Root Mean Square of Approximation (RMSEA) is also reported where values greater than 0.1 are taken as indicative of a poor fit of the data, the rule of thumb suggested by Browne and Cudeck (Reference Browne, Cudeck, Bollen and Long1993).
Prior to the multiple regression analyses, dependent and predictor variables were checked for multicollinearity by examination of an inter-item correlation matrix where values above 0.80 (Field, Reference Field2000, p. 132), VIF >10 (Myers, Reference Myers1990), and tolerance statistics <0.1 (Bowerman and O'Connell, Reference Bowerman and O'Connell1990) would suggest that multicollinearity was a problem. Predictor variables were checked for independent residuals using Durbin-Watson test statistic (Durbin and Watson, Reference Durbin and Watson1951) where values <1 or >3 would indicate residuals were correlated. They were also checked for the presence of outliers and extreme cases of residual statistics by examination of standardized residuals for values >3, Cook's distance for values >1 (Cook and Weisberg, Reference Cook and Weisberg1982), which would indicate the model was a poor fit of the data and that outliers may be present. Linearity and homoscedasticity were checked by the examination of standardized residual scatterplots; finally histograms and normal probability plots were examined to check for normally distributed residuals as recommended by Field (Reference Field2000, p. 158).
The dependent variables, frequency of paranoid thoughts and distress about paranoid thoughts and the predictor variables were each entered into two multiple regression analyses: hierarchical, then stepwise. The hierarchical method was selected because it was of interest to investigate the contribution of the new predictors (BaPS) to the predictors that have existing support in the literature of their relationship to paranoia. Stepwise was selected because the hierarchical models included several non-significant coefficients, indicating that these variables did not contribute much to the model. The stepwise method of model selection resulted in only significant predictors added into the regression equation and a smaller but significant model of predictors. The order of measures entered into the regression was age and gender, self-consciousness, anxiety and depression, thought control and then beliefs about paranoia. We wished to enter the measures in this way in order to ensure that other explanatory variables were controlled for before evaluating the contribution of beliefs about paranoia. Both hierarchical and stepwise models are presented. Based on Green (Reference Green1991) the number of participants required was calculated on basis of N > 50 + 8x where x = n of independent variables (n = 15) the required sample size to test the variables selected for our model was 170.
Results
Participant characteristics
The number or participants completing the questionnaires was 185. The mean age of the group was 23.17 (SD = 6.13; range 17–39 years). The male: female ratio was 39:142 (data missing for seven cases). Descriptive data from the standardized measures are presented in Table 1.
Table 1. Descriptive statistics from standardized measures

Four factor model
Examination of the inter-item correlation matrix revealed a predominance of correlations above 0.3 among the items supporting suitability for factor analysis. The Kaiser-Meyer (KMO) measure provides a further means for assessing the homogeneity of variables. The overall KMO measure was 0.89, which was above the suggested minimum of 0.60 (Tabachnick and Fiddell, Reference Tabachnick and Fidell1996), indicating that the correlation matrix was suitable for factoring. Eight items (items 10, 12, 18, 30, 37, 39, 41, and 50) of the BaPS showed a limited range of endorsements, with more than 80% of scores in the “not at all category”. Therefore, two confirmatory factor analyses were performed with and without items with frequency problems. Both the original 50-item questionnaire and then the 42-item questionnaire, where the eight items with frequency problems were removed, proved to be a poor fit of the data (χ2 = 1052.10, p < .00; χ2 = 6048.43, p < .00). The CFI were 0.70 and 0.77 and the RSMEA were 0.11 and 0.11. It was therefore appropriate to examine the possible structure of the observed correlations using exploratory factor analysis.
Having removed the eight problematic outcomes, a Principal Components Analysis was performed on the 42 items in order to reduce the variables to a smaller number of components by examining the Scree plot (Cattell, Reference Cattell1966) and percentage of variance explained. The Scree test revealed a clear break in slope between four and five factors; therefore four factors were specified in a maximum likelihood factor analysis using a varimax rotation. The rotated loadings indicated that the fourth factor was problematic, with only three items from the original hypothesized “interesting beliefs” factor loading highly. The fourth item “people who are not paranoid are just not getting it” was originally from the “normalizing beliefs” factor and therefore did not load onto its original factor as expected. All of the four items loading onto factor four had frequency problems. The four factors explained 31.53 (F1), 12.13 (F2), 8.4 (F3) and 4.0 (F4) per cent of the variance.
Three factor model
There were several reasons for rejecting the original 4-factor model. An inadequate fit of the 4-factor model was demonstrated by CFA. There were frequency problems for the four items that loaded onto the fourth factor. In addition, many of the original items that were constructed for factor four appeared ambiguous and therefore difficult for respondents to answer. Therefore the selection of a 3-factor model was deemed appropriate. A maximum likelihood factor analysis was performed using varimax rotation specifying three factors with all items originally constructed for factor four omitted from this analysis. The first three factors had the following eigenvalues: 12.79, 5.22, and 3.65 and explained 32.76 (F1), 13.40 (F2) and 9.37 (F3) per cent of the variance. Thereafter, the eigenvalues for the next three components were 1.31, 1.16 and 1.02. A CFA was performed on this 38-item version of the BAPS, resulting in a better fit of the data on all indices apart from χ2, which remained significant (χ2 = 1432.5, p < .00; CFI = 0.81; RMSEA = 0.08). Finally, the six items with the highest loading on each factor were retained, resulting in an 18-item questionnaire comprising six items in each factor. A test of the 3-factor model indicated that although the chi-squared test of overall model fit remained significant (χ2 = 312.46, p < .00), the other indices indicated a good fit, with the RMSEA value now 0.9 and the CFI was 0.92. The χ2 is extremely sensitive with small variations in fit resulting in statistically significant and sizeable χ2 (Hu and Bentler, Reference Hu, Bentler and Hoyle1995). Despite this index, the abbreviated 3-factor model was deemed a good fit of the data. A summary of the results from all the confirmatory factor analyses are presented in Table 2.
Table 2. Fit indices for CFA models of the BaPS

Internal consistency of the BAPS (18 item)
Internal consistency was examined for the 18-item BaPS using Cronbach's alpha computed for the total scale and the three subscales. The scale demonstrated good internal consistency with alphas of 0.89; 95% CI = 0.87 – 0.91 (FI), 0.90; 95% CI = 0.87 – 0.92 (F2); 0.93; 95% CI = 0.91 – 0.94 (F3); and 0.89; 95% CI = 0.87 – 0.91 for the total scale. Items and their loadings for the 3-factor model are presented in Table 3.
Table 3. Factor loadings of the BAPS (three-factor model) from Maximum Likelihood Factor Analysis using varimax rotation
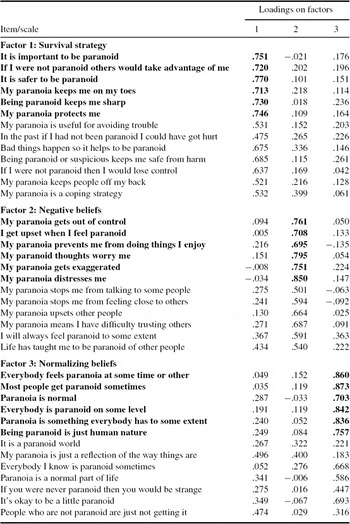
(Items emboldened were retained to form the 18 item BAPS).
Predictors of frequency of and distress about paranoia
The examination of the inter-item correlation matrix and tolerance index indicated that multicollinearity was not a problem. All assumptions necessary for multiple regressions were met. Hierarchical (blockwise entry) and stepwise multiple regression analyses were performed to examine the hypotheses that paranoia frequency is associated with positive beliefs about paranoia, punishment, worry and reappraisal thought control strategies and negative beliefs about paranoia are associated with higher distress about paranoia in a non clinical sample. For hierarchical models, the predictor variables were entered in the following order: SCS subscales; HADS subscales; TCQ subscales; and finally the BAPS subscales. The correlation matrix for all predictor and outcome variables and the results of the multiple regression analyses for paranoia frequency and paranoia distress are presented in Tables 4, 5, and 6 respectively.
Table 4. Correlation matrix for paranoia frequency, paranoia distress and predictor variables
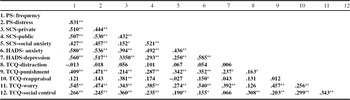
**Correlation is significant at the 0.01 level (2-tailed); *Correlation is significant at the 0.05 level (2-tailed).
Table 5. Multiple regression statistics for paranoia frequency

*The standardized regression coefficient or beta and the partial correlation are shown, which indicated the importance of the independent contribution of each variable at the final stage of analysis to the prediction of paranoia frequency when all other predictors are held constant.
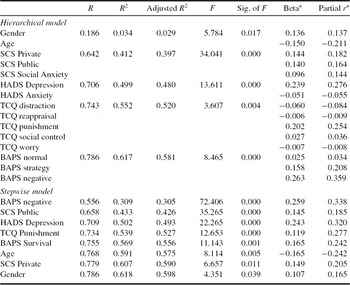
Table 6. Multiple regression statistics for paranoia distress

*The standardized regression coefficient or beta and the partial correlation are shown, which indicated the importance of the independent contribution of each variable at the final stage of analysis to the prediction of paranoia frequency when all other predictors are held constant.
Predictors of paranoia frequency
In the hierarchical method of multiple regression, on step 1 when age and gender were entered the multiple R was 0.157, R 2 was 0.025, adjusted R 2 was 0.019 and significant (F = 4.08, p = .045). On step 2, when the SCS variables were entered the multiple R was 0.651, R 2 was 0.423, adjusted R 2 was 0.409, and the increment in R 2 0.398 and significant (F = 36.41, p < .001). On step 3 when the HADS variables were entered the multiple R was 0.740, R 2 was 0.548, the adjusted R 2 was 0.530 and the increment in R 2 0.125 was significant (F = 21.47, p < .001). On step 4 when the TCQ variables were entered the multiple R was 0.774, R 2 was 0.599, the adjusted R 2 was .570, the increment in R 2 of 0.051 was significant (F = 3.85, p < .05). On the final step when the BAPS variables were entered, the multiple R was 0.818, the R 2 was 0.669, adjusted R 2 was 0.638 and the increment in R 2 of 0.070 was significant (F = 10.51, p < .001), showing that the addition of the BAPS items accounted for an additional 7.0% of the variance.
When all predictor variables (n = 15) were entered into the model, the stepwise method indicated that seven variables remained significant for inclusion into the model and accounted for 63% of the variance. BaPS-negative beliefs accounted for 34.5% of the variance with R 2 of 0.345, with a multiple R of 0.587. HADS depression accounted for an additional 13.8% of the variance with an increment in R 2 of 0.138, R 2 of 0.483 and multiple R of 0.695. SCS private accounted for an additional 6.7% of the variance with an increment in R 2 of 0.067, R 2 of 0.550, and a multiple R of 0.742. The multiple R for BaPS strategy was 0.771; R 2 was 0.594 with an increment of 0.029. Age accounted for 3.6% of the variance with an increment in R 2 of 0.036, R 2 of 0.630 and multiple R of 0.794. For TCQ-punishment the multiple R was 0.803, R 2 was 0.645 and increment of 0.015. For SCS Public, multiple R was 0.809, R 2 was 0.654, and adjusted R 2 was 0.639 with an increment of 0.009.
Predictors of paranoia distress
In the hierarchical method of multiple regression, on step 1 age and gender were entered the multiple R was 0.186, R 2 was 0.034 and adjusted R 2 0.029 and significant (F = 5.784, p < .05). On step 2 when the SCS variables were entered the multiple R was 0.642, R 2 was 0.412, the adjusted R 2 was 0.397, the increment of R 2 0.378 and significant (F = 34.04, p < .001). On step 3 when the HADS variables were entered the multiple R was 0.706, R 2 was 0.499, adjusted R 2 0.480, and increment in R 2 was 0.087 and significant (F = 13.61, p < .001). On step 4 when the TCQ variables were entered the multiple R was 0.743, R 2 was 0.552, adjusted R 2 was 0.520 and the increment in R 2 was 0.053 and significant (F = 3.607, p < .05). On step 5 when the BAPS variables were entered the multiple R was 0.786, R 2 was 0.617, the adjusted R 2 0.581 and the increment of 0.065 was significant (F = 8.465, p < .001).
When all predictor variables (n = 15) were entered into the model, the stepwise method indicated that eight variables remained significant and accounted for 61.8% of the variance. BaPS-negative accounted for 30.9% of the variance, with a multiple R of 0.556, and R 2 of 0.309. For SCS public, the multiple R was 0.658, R 2 was 0.433, adjusted R 2 was 0.426 and the increment in R 2 was 0.124. For HADS depression, the multiple R was 0.709, R 2 was 0.502, adjusted R 2 was 0.493 and the increment in R 2 was 0.069. TCQ punishment had a multiple R of 0.734, R 2 0.539, adjusted R 2 0.0.527 with an increment of 0.037. BaPS Survival had a multiple R of 0.755, R 2 of 0.569, and adjusted R 2 of 0.556 with an increment of 0.030. Age had a multiple R of 0.768, R 2 of 0.591, adjusted R 2 of 0.575 and increment of 0.022. SCS Private had a multiple R of 0.779, R 2 of 0.607, adjusted R 2 of 0.590 and increment of 0.016. Gender had a multiple R of 0.786, R 2 of 0.618, adjusted R 2 of 0.598 and increment of 0.011.
Discussion
The purpose of this study was to investigate the role of beliefs about paranoia as predictors of frequency and distress of paranoia in a non-clinical population. The results of the empirical validation of the 50-item BaPS demonstrated that the original BaPS, which hypothesized a 4-factor solution, was a poor fit of the data. This was demonstrated in confirmatory and exploratory factor analyses. The final 18-item BaPS was found to demonstrate good internal reliability. The 18-item BaPS measured three distinct subscales regarding beliefs about paranoia. Despite the rejection of the fourth factor, general positive beliefs, the three factors survival beliefs, normalizing beliefs and negative beliefs were found to be distinct factors measured by the BaPS. There is an important need to replicate these findings regarding the 3-factor structure of the BaPS, preferably in a clinical population.
Our hypothesis that positive beliefs about paranoia would be associated with paranoia frequency was not fully supported. Whilst we found that positive beliefs about paranoia as a survival strategy were selected as a predictor of paranoia frequency in the stepwise model, this effect was small and the negative beliefs about paranoia predicted a larger proportion of the variance (34.5% versus 2.9%). This was an interesting finding, which opens up further understanding of a metacognitive conceptualization of paranoia. These findings suggest an important role for negative beliefs about paranoia playing an important role in the prediction of the frequency of paranoid thoughts. It may be that negative beliefs about paranoia are associated with increased vigilance towards paranoid thoughts as a source of threat, thus increasing attentional deployment towards thoughts and images concerning interpersonal threat. This finding is potentially consistent with Wells' (Reference Wells1995) metacognitive model of worry, where negative beliefs about worry lead to increased ruminative focus on worry related thoughts. Furthermore, similar negative metacognitive beliefs are associated with predisposition to hallucinations in non-clinical and clinical samples (Morrison, Wells and Nothard, Reference Morrison, Wells and Nothard2002; Baker and Morrison, Reference Baker and Morrison1998). In a clinical group of 27 individuals diagnosed with schizophrenia, we found that negative beliefs about paranoia were associated with increased re-experiencing of traumatic memories linked to Post Psychotic PTSD (White and Gumley, Reference White and Gumley2009). We also found that negative beliefs about paranoia were associated with increased intolerance of uncertainty, a construct closely associated with worrying (White and Gumley, in press).
We also observed that public and private self-consciousness were also significant predictors of paranoia frequency. Fenigstein and Vanable (Reference Fenigstein and Vanable1992) found that high levels of public self-consciousness in non-clinical participants were associated with paranoia frequency. Self-consciousness is suggested to increase the extent to which participants perceive another's behaviour as being directed towards them (Fenigstein, Reference Fenigstein1984). The finding that frequency of paranoid ideation is related to self-consciousness is therefore not unexpected and is consistent with the hierarchical account of paranoid thinking as described by Freeman et al. (Reference Freeman, Garety, Bebbington, Smith, Rollinson, Fowler, Kuipers, Katarzyna and Dunn2005a). The finding that depression was also a significant predictor of paranoia frequency is also of interest. On the one hand, this may well be consistent with a negative ruminative focus which has been observed in depression and which was suggested by the findings for negative beliefs about paranoia. On the other hand, the Fenigstein Scale has been criticized as some of the items are negatively affectively valenced (Freeman et al., Reference Freeman, Garety, Bebbington, Smith, Rollinson, Fowler, Kuipers, Katarzyna and Dunn2005a). It may be that the finding that HADS depression predicts frequency of paranoia is a reflection of overlapping items. We also note that the Fenigstein Scale was originally designed as a trait measure of paranoia. More recently the Paranoid Thoughts Scale (Freeman et al., Reference Freeman, Garety, Bebbington, Smith, Rollinson, Fowler, Kuipers, Katarzyna and Dunn2005a) has been developed and this may well have been a better measure of frequency of paranoid thoughts. We also note that the restricted range of variance indicated by low scores on Fenigstein Scale and the low score on HAS depression scale may also have increased the magnitude of association observed in this analysis.
The hypothesis that negative beliefs concerning appraisals of uncontrollability, exaggeration, worry and distress in relation to paranoid thoughts would be associated with distress about paranoia gained substantial support. This finding is consistent with Freeman and Garety (Reference Freeman and Garety1999) who found a positive association between delusional distress and the individual's experiences of meta-worry concerning the control of delusion related worries. This is supportive of the metacognitive prediction of the S-REF model (Wells and Mathews, Reference Wells and Matthews1994) that metacognitive beliefs about mental experiences are associated with vulnerability to psychological disorder, and confirms the suggestion that negative beliefs about paranoia are associated with distress in response to paranoid ideation (Morrison et al., Reference Morrison, Gumley, Schwannauer, Campbell, Gleeson, Griffin and Gillan2005).
Punishment was also found to be a significant predictor of paranoia frequency. Although worry was a non-significant predictor, the finding that distraction had a negative relationship with paranoia frequency is supportive of the finding that patients experiencing delusional beliefs and hallucinations used more punishment and worry and less distraction thought control strategies compared to non-patients (Morrison and Wells, Reference Morrison and Wells2000). Overall, these findings are consistent with the S-REF model's (Wells and Mathews, Reference Wells and Matthews1994) prediction that metacognitive dysfunctional plans for processing, such as use of punishment, are related to emotional dysfunction maintenance.
This study has several methodological limitations that require to be addressed. Although analogue research is increasingly being used in the field of psychosis research (e.g. Morrison et al., Reference Morrison, Wells and Nothard2002; Morrison and Petersen, Reference Morrison and Petersen2003), the use of non-clinical participants limits generalizability of findings to clinical populations. It cannot be assumed that the same metacognitive processes are operating in clinical populations. However, this study was investigating metacognitive beliefs and processes involved in sub-clinical levels of paranoia. Combs, Penn and Fenigstein (Reference Combs, Penn and Fenigstein2002) argues that the assessment of sub-clinical paranoia is important, as demonstrated by current conceptualizations of psychosis, such as that of Bentall, Jackson and Pilgrim (Reference Bentall, Jackson and Pilgrim1988), where symptoms are described as existing on a continuum, as opposed to separate, categorical entities. It may be argued that the identification of metacognitive processes operating in non-clinical paranoia will enable the identification of variables involved in the transition to clinical paranoia.
Further limitations concern the use of a correlational, cross sectional design, which prevents inferences of causality being made. It is suggested that eliciting the causal role of metacognitive beliefs in predisposition to paranoia and distress would involve longitudinal or experimental designs. Furthermore, the current study utilised a convenience sample; this limits the potential to assess the generalizability of these findings (Robson, Reference Robson1993, p. 72). A consequence of convenience sampling is that caution is required when attempting to make statistical inferences about other populations from the responses of this population. Another limitation was that the sample was predominantly female and it is possible that the findings were influenced by gender.
This study would have been enhanced by investigation of physiological effects of factors such as drug use and sleep deprivation, both of which are suggested as being implicated in the development and maintenance of psychosis symptoms (Morrison et al., Reference Morrison, Gumley, Schwannauer, Campbell, Gleeson, Griffin and Gillan2005). There is increasing evidence that cannabis may induce paranoid phenomena such as delusions, for example (Mathews, Wilson, Humphreys, Lowe and Weithe, Reference Mathews, Wilson, Humphreys, Lowe and Weithe1993), and this study did not investigate this. In addition, there was no investigation of traumatic life experiences, which have an association with the themes expressed in psychosis phenomena, such as delusions (Raune, Kuipers and Bebbington, Reference Raune, Kuipers and Bebbington1999).
It is also important to acknowledge that in no way did we seek to offer participants a specific definition of paranoia. This was so as not to constrain their participation in the study. This in itself is also a methodological limitation in that we are not able to be sure that our participants would construct paranoia in the same way as clinical participants. We are encouraged, however, that our findings in this study are consistent with our findings from initial clinical studies where negative beliefs about paranoia are associated with persecutory delusions (Morrison et al., in press), re-experiencing of traumatic memories of psychosis (White and Gumley, Reference White and Gumley2009) and greater propensity towards worrying as reflected in Intolerance of Uncertainty (White and Gumley, in press).
Future research is required to assess the application of the BaPS with clinical populations. In addition, the sensitivity of the BaPS to therapeutic change remains to be examined. The metacognitive model presented in this study will be enhanced by further understanding of cognitive responses involved in maintenance that are unique to paranoia. Furthermore, we hypothesize that Beliefs about Paranoia are linked to the strategic deployment of attentional resources towards thoughts and images concerning interpersonal threat. This model assumes that paranoid thoughts are normally occurring (Freeman et al., Reference Freeman, Garety, Bebbington, Smith, Rollinson, Fowler, Kuipers, Katarzyna and Dunn2005a). It is also important to distinguish beliefs about paranoia from the moment by moment interpretations of paranoid thoughts, which may be highly idiosyncratic or linked to other emotional responses including shame, embarrassment and stigma. The TCQ was used for this purpose and it was originally developed for use with intrusive thoughts, and not for use with psychosis phenomena. Further development of standardized measures of metacognitive processes involved in maintenance of paranoia is required.
The development of a metacognitive model of paranoia has several important implications for clinical practice. First, one of the targets of assessment will be an examination of the positive beliefs that an individual holds in relation to their paranoia. If the individual views paranoia as a survival strategy, then it is paramount that they are provided with an alternative, functional, replacement strategy. Second, treatment will be enhanced by the identification of the negative beliefs the individual holds about their paranoid thoughts, as suggested by Morrison, Renton, Dunn, Williams and Bentall (Reference Morrison, Renton, Dunn, Williams and Bentall2003). This will assist in reducing associated distress. Third, the identification of dysfunctional coping strategies, such as use of punishment thought control, will enable the maintenance of the individual's paranoia to be targeted. This is essential for the long-term success of cognitive therapy with paranoia.






Comments
No Comments have been published for this article.