


Introduction
Clark and Wells (Reference Curtis and Miller1995) proposed a cognitive model of social phobia that attempts to explain the maintenance of the disorder, and account for why individuals with social phobia fail to benefit from the naturalistic exposure that is provided by their everyday interactions with other people. In this model, social phobia is seen as resulting from problematic beliefs about oneself and one's social world, which lead individuals with social phobia to interpret social situations in an excessively negative fashion. Negative interpretations (danger appraisals) are then maintained by the four processes outlined below. The first is (a) increased self-focused attention, which is linked to a decrease in the observation of other people and their responses. The individual may also (b) use misleading internal information (feelings and self-images) to make excessively negative inferences about how they appear to others. They may extensively use (c) safety behaviours (including overt avoidance) that are intended to prevent feared catastrophes, but that have the consequences of maintaining negative beliefs, increasing feared symptoms, and making the individual come across to others in ways that are likely to elicit less friendly responses. Finally, the individual may (d) engage in negatively biased pre and post-event processing. In this model safety behaviours are conceptualized as anything the individual does or avoids doing in order to prevent their social fears from being realized. For example, someone who fears other people noticing how anxious they are in social situations may use overt avoidance, such as avoiding social situations or not speaking in the situation. Alternatively, they may use more subtle forms of avoidance, such as avoiding eye contact or planning and rehearsing what to say, in order to prevent their fear of appearing anxious from being realized. See Figure 1 for a summary of the model.
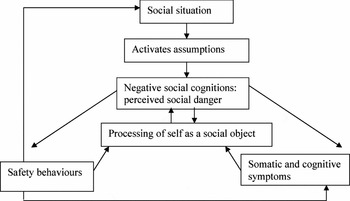
Figure 1. Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model of social phobia
There is empirical support for most of the hypotheses embedded within Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) model (see Clark, Reference Clark, Crozier and Alden2001 for a review). The model has been used to develop a 14-session cognitive therapy protocol for treating social phobia in adults, which has been demonstrated to have particularly large effect sizes in a number of randomized controlled trials (Clark et al., Reference Clark, Wells, Heimberg, Liebowitz, Hope and Schneier2003, Reference Curtis and Miller2006; Stangier, Heidenreich, Peitz, Lauterbach and Clark, Reference Clark, Ehlers, McManus, Hackmann, Fennell, Campbell, Flower, Davenport and Louis2003).
The prevalence of childhood social phobia has been reported to be as high as 13.3% (Kessler et al., Reference Kovacs1994), and when social anxiety remains untreated in younger people it is associated with debilitating consequences such as failing to complete education, avoidance of age-specific social activities such as dating and seeking employment, and loneliness and isolation (Albano and Detweiler, Reference Albano, Detweiler, Hofmann and DiBartolo2001). Hence, it remains a priority to establish working models of social anxiety in young people so that effective treatments can be developed for this population.
Despite the high prevalence and debilitating consequences of childhood social phobia, there is a relative paucity of research into the causes or cures of social anxiety in young people. Most research into social anxiety in children has concentrated on identifying social skills deficits and utilizing social skills training programs (e.g. Spence, Donovan and Brechman-Toussaint, Reference Spence, Donovan and Brechman-Toussaint2000). However, it may be that any observed skills deficits can be explained within a cognitive-behavioural framework. For example, it is possible that socially anxious young people's use of safety behaviours contaminates their social performance. Some support for this proposition comes from studies on adults showing that social fears (in particular the belief that the other person will appraise you negatively) and the consequent use of more safety behaviours leads to less acceptable social behaviour (Alden and Beiling, Reference Alden and Bieling1998; Curtis and Millar, Reference Curtis and Miller1986; McManus, Sacadura and Clark, in press).
More recent research in childhood social anxiety has concentrated on looking at the role of negative social cognitions (e.g. Bogels and Zigterman, Reference Bogels and Zigterman2000; Rheingold, Herbert and Franklin, Reference Rheingold, Herbert and Franklin2003) and some authors have concluded that rather than performing more negatively, socially anxious children simply fear that they have performed more negatively (Cartwright-Hatton, Hodges and Porter, Reference Cartwright-Hatton, Hodges and Porter2003) and hence have called for such social fears to be addressed through the use of cognitive behavioural techniques (Cartwright-Hatton, Tschernitz and Gomersall, Reference Cartwright-Hatton, Tschernitz and Gomersall2005).
Given the recent focus on the role of cognitive factors in childhood social phobia, it seems sensible to test the applicability of Clark and Wells's (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model, which has been used to effectively conceptualize and treat social phobia in adult populations.
In the broader research literature there are examples of cognitive models that have been developed for adult populations being successfully applied to younger populations. For example, Stallard (Reference Stangier, Heidenreich, Peitz, Lauterbach and Clark2003) tested Ehlers and Clarks’ (Reference Ehlers and Clark2000) cognitive model of PTSD, that was developed from studies on adult populations, with traumatized children and found support for four out of the five variables, namely: trauma severity, sequelae appraisal, behavioural avoidance, and cognitive strategies. Smith et al. (Reference Spence, Donovan and Brechman-Toussaint2004) then tested the treatment arising from this model with children who were suffering from PTSD with positive results. Thus cognitive models developed for adult populations have been shown to have validity for younger populations and the treatments developed from them have been successfully applied to young people with similar anxiety disorders. Hence, this study aims to test the validity of Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model of social phobia for younger people, in order to inform the development of future treatment protocols for this group, particularly given the large effect sizes for interventions based on this model in adult populations.
Thus the current study aimed to examine whether the variables in Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) model were more evidenced in “high” socially anxious young people than in “low” socially anxious young people, and whether they predicted social anxiety over and above a general mental health problem, such as depression. More specifically, the following hypotheses were tested:
• The “high” social anxiety group would score significantly higher than the “low” social anxiety group on measures of the variables from Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model of social phobia (namely: negative social cognitions, safety behaviours, self-focused attention, and pre and post-event processing).
• Each of the variables in Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model would individually predict social anxiety.
• The variables in Clark and Wells' (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model would predict significantly more of the variance in social anxiety than in depression.
Method
Participants and procedure
Participants were 11 to 14-year-olds (N = 171, mean age = 12.24 years, SD = 0.97) recruited from three local secondary schools within the UK. No participants over the age of 14-years were recruited for this study, as the SPAI-C has only been validated in young people up to and including 14-years. Ninety-five participants (56%) were female. After informed consent had been obtained from both the participant and their parent, participants completed a booklet of questionnaires during a lesson at school. If willing, participants were asked to complete a sub-set of the questionnaires (those that did not have established psychometric properties for use with young people) 2 weeks later, to establish the test-retest reliability of these measures.
Measures
The Social Phobia and Anxiety Inventory for Children (SPAI-C; Beidel, Turner and Morris, Reference Beidel, Turner and Morris1995) The SPAI-C, which was used as the main outcome measure, is a 26-item measure of the somatic, cognitive and behavioural aspects of social phobia in children aged 8 to 14-years. It has good internal consistency (alpha = 0.92), discriminative validity, and test-retest reliability (Beidel, Turner and Fink, Reference Beidel, Turner and Fink1996).
Social Behaviour Questionnaire (SBQ; Clark et al., Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) The SBQ requires participants to rate how frequently they engage in 28 social anxiety-related safety behaviours. These include behaviours such as rehearsing what to say, checking that you are coming across well, and avoiding eye contact. For the purposes of this study the item referring to using alcohol to manage anxiety was removed as it was unlikely to be relevant to younger participants. Although the SBQ has not been validated for use with young people it was chosen as no validated measure of social anxiety related safety behaviours exists for young people. Studies using the SBQ with adult samples report high levels of internal consistency (e.g. McManus et al., in press, Cronbach's alpha = 0.88).
Social Cognitions Questionnaire (SCQ; Wells, Stopa and Clark, Reference Wells, Stopa and Clark1993) The SCQ lists 22 social anxiety-related fears, such as the thinking that you will blush or that others will think you boring, and asks for ratings of how frequently the respondent has had that thought in the last week. Although the SCQ has not been validated for use with young people, it was chosen as no validated measure exists. Studies using the SCQ with adult samples report high levels of internal consistency (e.g. McManus et al., in press, Cronbach's alpha = 0.95).
Focus of Attention Questionnaire (FAQ; Woody, Reference Woody1996) The FAQ consists of two 5-item subscales: self-focused attention and other-focused attention. For example, respondents rate how much they were “focusing on their level of anxiety” or how much they were “focusing on what they thought of another person” in a social situation. The FAQ has not been validated for use with young people, but both the sub-scales have acceptable internal consistency (alpha = 0.76 and 0.72 for self and other focus respectively) in a sample of adults with social phobia (Woody, Chambless and Glass, Reference Woody, Chambless and Glass1997).
Post Event Processing questionnaire (PEP; Rachman, Gruter-Andrew and Shafran, Reference Rachman, Gruter-Andrew and Shafran2000) This 13-item questionnaire focuses on post-event processing after social situations. Respondents are asked to rate on a 1–100 scale how much they processed the event after it was over e.g. whether they found themselves thinking about the event after it was over and whether they found it difficult to forget about the event. The PEP has not been validated for use with children but was chosen because no other measures exist for post-event processing in young people. Studies using the PEP with adult samples report high levels of internal consistency (e.g. Rachman et al., Reference Rheingold, Herbert and Franklin2000 report Cronbach's alpha of 0.85).
Social Phobia Weekly Summary Scale (SPWSS; Clark et al., Reference Clark, Ehlers, McManus, Hackmann, Fennell, Campbell, Flower, Davenport and Louis2003) Items 3, 4 and 5 were used from this 5-item scale, which examined the degree of participants’ self-focused attention, pre and post-event processing over the previous week. The SPWSS has satisfactory internal consistency (Cronbach's alpha = 0.81) and has been used as an outcome measure in treatment trials of social phobia in adult populations (e.g. Clark et al., Reference Clark, Wells, Heimberg, Liebowitz, Hope and Schneier2003, Reference Curtis and Miller2006).
Birleson Depression Self-Rating Scale (DSRS; Birleson, Hudson, Buchanan and Wolff, Reference Birleson, Hudson, Buchanan and Wolff1987) The DSRS is a widely used 18-item measure of the cognitive and somatic symptoms of depression in young people. The DSRS is well validated, has been found to correlate highly with other measures of childhood depression (e.g. Kovacs, Reference Ivarsson, Lidberg and Gillberg1992), and is easy to administer (Birleson et al., Reference Birleson, Hudson, Buchanan and Wolff1987) and has good psychometric properties with adolescent samples (e.g. Ivarsson, Lidberg and Gillberg, Reference Ivarsson, Lidberg and Gillberg1994 reported Cronbach's alpha = 0.90).
The second, shorter questionnaire pack contained the measures that did not have established psychometric properties for use with young people, namely the SBQ, SCQ, FAQ, PEP and the SPWSS.
Statistical methods
Data were analysed using SPSS (v14.0) and will be presented throughout as mean (SD). Statistical significance was taken at the 5% level (p <. 05). Cronbach's alpha coefficients were calculated to assess the internal consistency of the questionnaires. Values of alpha in the range 0.80 to 0.90 are considered optimal (Guyatt, Feeny and Patrick, Reference Guyatt, Feeny and Patrick1993), with a minimum alpha of 0.70 being necessary to claim internal consistency (Nunnally and Bernstein, Reference Rachman, Gruter-Andrew and Shafran1994). The test-retest properties of the measures were examined using Pearson and Spearman correlations. Paired t-tests were used to compare the scores on the two occasions.
A quartile split was used to form “high” and “low” socially anxious groups, on the basis of the highest and lowest 25% of SPAI-C scores. The participants scoring the middle 50% of scores on the SPAI-C were labelled “middle” anxiety group. “Socially anxious” and “non-socially anxious” groups were also formed using the recommended clinical cut-off of 18 or above on the SPAI-C, and an identical pattern of results was obtained. To save repetition, however, only the results from the quartile split method will be reported. The groups were compared using either chi-squared (χ2) tests for categorical data, and one-way analysis of variance (ANOVA) for continuous data.
When comparing the “high”, “middle” and “low” social anxiety group on measures of the variables from Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model of social phobia, a one-way ANOVA was used with post-hoc Tukey tests to identify individual significant differences. In terms of comparisons across childhood, in order to have sufficient numbers for comparison, a “younger” and “older” age group were used, with the former being composed of 11 to 12 year olds (N = 95), and the latter being 13 to 14 year olds (N = 72). Independent sample t-tests were used to compare the groups.
To determine which variables predict social phobia, simple linear regression analyses were undertaken between each of the five variables identified by Clark and Wells' (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) model and the SPAI-C score, on data from all 171 participants.
Multiple regression analyses were used to compare the power of the variables from Clark and Wells' (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) model to predict social anxiety with their power in predicting depression. In the first analysis, the dependent variable was social anxiety (SPAI-C), and the 5 variables from the cognitive model were all entered into the analysis (scores for safety behaviours, negative social cognitions, focus of attention, post-event, and pre-event processing). In the second analysis, depression (DSRS) was the dependent variable, although the procedure and the independent variables were both identical to the first analysis. Stepwise regression analysis with the above 5 variables entered as potential predictor variables was used to identify the variables that were independently predictive of both social anxiety and depression. The model with social anxiety as the dependent variable was run with and without adjustment for depression score.
Results
Psychometric properties of questionnaires
The SCQ, SBQ, PEP and FAQ all showed “high” internal consistency in this sample (e.g. alpha values ranged from 0.82 to 0.94). The SPWSS showed lower internal consistency than the other measures (alpha = 0.71), which is not surprising given that the 5 items in the SPWSS are intended to measure 5 different constructs. In terms of test-retest reliability, with the exception of the SBQ, there were no significant differences in the questionnaire scores on the two occasions they were completed. Participants scored significantly higher on their first completion of the SBQ than on their second completion (means = 29.34 (9.19) vs 26.10, (9.01); t = 2.26, p = .03).
High versus low socially anxious groups
Scores on the SPAI-C ranged from 0 to 44 with mean SPAI-C score of 12.19 (SD = 8.12), which was below the clinical cut-off indicative of social phobia (Beidel et al., Reference Beidel, Turner and Fink1996). The high socially anxious group (N = 47) had a mean score of 22.4 (SD = 5.89) on the SPAI-C, and 70.2% (N = 33) scored above the clinical cut-off recommended to indicate the presence of social phobia (Beidel et al., Reference Beidel, Turner and Fink1996). The mean SPAI-C score for the middle socially anxious group (N = 76) was 11.29 (SD = 2.79), and the mean SPAI-C score for the low socially anxious group (N = 48) was 3.5 (SD = 2.03). All participants from the middle and low socially anxious group scored within the non-clinical range. There were no significant differences between the groups in gender, age or ethnicity (respectively x2 = 1.03, p = .60; F= 0.24, p = .79, x2 = 16.38, p = .09).
Comparing the high, middle, and low social anxiety group on measures of the variables from Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model of social phobia
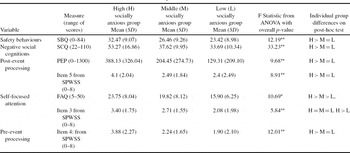
Participants within the high, middle and low socially anxious groups scored significantly differently on safety behaviours, negative social cognitions, post-event processing, pre-event processing and self-focused attention (see Table 1 for a comparison of means). More specifically, post-hoc tests demonstrated that the high socially anxious group scored significantly higher on all five variables within Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model, compared to the low socially anxious group (as all p values were less than 0.01).
Table 1. Difference between the high, middle and low socially anxious groups on the variables from Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model of social phobia
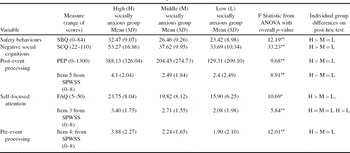
*= p < .01;** = p < .001 > significantly greater than = not significantly different.
Do the variables from Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model change across childhood?
There were no significant differences between the two age groups in gender or ethnicity (respectively x2 = 0.03, p = .49; x2 = 1.73, p = .15). The mean SPAI-C score for the younger group was 11.59 (SD = 7.62) and the mean SPAI-C score for the older group was 12.97 (SD = 8.73), which were not significantly different (t = −1.09, p = .28), and were under the clinical cut-off to indicate the presence of social phobia (Beidel et al., Reference Beidel, Turner and Fink1996). There were also no significant differences (t = 0.14, p = .89) in the mean depression score for the younger and older groups (respectively 9.45 (SD = 5.35) and 9.34 (SD = 4.82)). Thus no further analyses will be reported between the two age groups.
Do all the variables predict social phobia?
The individual regression analyses suggested that when considered in isolation, each of the five variables were predictive of social anxiety (see Tables 2 and 3).
Table 2. Linear regressions between SPAI-C and depression score (the dependent variables) and the other measures from Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model, showing the values of R2, the regression coefficients, and the F statistics for each model
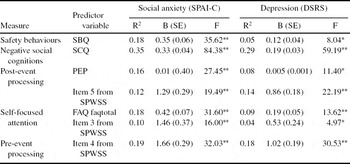
* = p<.01; ** = p<.001.
Table 3. Results of stepwise linear regressions showing the measures from Clark and Well's model that are independently predictive of both social anxiety and depression. Values of the regression coefficients and their p-values are given for each model

*Pre-event processing entered the model (p = .029) when post-event processing was excluded. The model was similar when adjustment was made in the model for depression score.
Are the variables from Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model specific to childhood social anxiety?
The R2 from the first multiple regression analysis, in which social anxiety was the dependent variable (and all five variables were forced in), was 0.48, which was significant (p<.001). In the second analysis, when depression (DSRS) was the dependent variable (and everything else remained unchanged), the results were as follows: R2 was 0.34, which was significant (p<.001). The R2 values for depression and social anxiety were then compared, and found to be significantly different (F = 45.23, p<.001). Thus, whilst the variables from Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model significantly predicted both depression and anxiety, they were significantly more predictive of social anxiety than they were of depression.
On a stepwise regression analysis with the above 5 variables entered as potential predictor variables, negative social cognitions was a significant independent predictor of both depression and social anxiety, entering each model first (p<.001). Post-event processing and self-focused attention were additional independent predictors of social anxiety (with and without simultaneous adjustment for depression score), and pre-event processing was an additional independent predictor of depression (Table 3). Excluding post-event processing from the list of predictor variables for social anxiety led to the addition of pre-event processing into the regression model.
Discussion
The results of this study suggest that Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model of social phobia may be applicable to young people with the condition, and that it has some specificity in predicting social anxiety over and above other childhood mental health disorders, such as depression. The results from the comparisons of those with high and low levels of social anxiety, and from the simple regression analyses, indicate that negative social cognitions, safety behaviours, self-focused attention and pre and post-event processing are all predictive of social anxiety in young people. The results from this study are thus consistent with previous research suggesting a cognitive component to social phobia in young people (e.g. Bogels and Zigterman, Reference Bogels and Zigterman2000; Cartwright-Hatton et al., Reference Cartwright-Hatton, Hodges and Porter2003; Rheingold et al., Reference Smith, Yule, Perrin, Tranah, Dalgleish and Clark2003).
Some tentative clinical implications arise from this study. The results suggest that Clark and Wells' (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model may have some validity for young people with the condition and hence the next steps would be to test the validity of this model in a treatment-seeking clinical population of socially phobic young people, and to begin to use the model as a template to guide assessment, formulation and treatment in this group. The results from this study suggest that it may be important to tackle all the variables highlighted as maintaining processes in the model. Clark et al.'s (Reference Clark, Ehlers, McManus, Hackmann, Fennell, Campbell, Flower, Davenport and Louis2003) protocol for treating social phobia in adult populations outlines strategies for reversing these hypothesized maintaining factors.
Given the high prevalence rate of childhood social phobia (e.g. 19.3% of the participants in this study scored above the clinical cut-off on a questionnaire measure of social phobia), it may be beneficial for preventative interventions to be undertaken in high risk populations. For example, school interventions, such as providing education on social anxiety, and normalizing anxiety responses. This would be in line with previous programs that have yielded significant effects by intervening with high risk individuals to prevent the onset of clinical disorder (e.g. Morrison et al., Reference Nunnally and Bernstein2004) or with programs that aim to modify the school environment or teach skills to promote mental health and/or prevent the deterioration from social anxiety to diagnosable social phobia (e.g. Fisher, Masia and Klein, Reference Fisher, Masia and Klein2004, or see Durlak and Wells, Reference Durlak and Wells1997 for a review).
It is worth noting that the current study has a number of limitations. As there are no established measures currently available to measure the constructs in Clark and Wells' (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) model in young people, the data in this study were obtained from questionnaires that were primarily developed for use with adults. Five of the questionnaires used did not have established psychometric properties for their use with under-18s. Nevertheless the measures did show high or acceptable internal consistency and all but the SBQ showed test-retest reliability. The SBQ was scored higher on first completion, and this may reflect the fact that it was the first measure to be completed out of the packs, so participants may have been experiencing higher levels of state anxiety at this point, because of the demands of the task. By the time of the second completion, participants were familiar with the procedure and the questionnaires, and hence may have scored lower on this questionnaire. Nevertheless, the SBQ may not be a valid measure of the safety behaviours in young people, so future research is needed to establish psychometric data for this measure or, preferably, to develop and validate a measure of safety behaviours specifically for younger populations.
The absence of more open-ended probes from the study may mean that any differences in how the variables from Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model are expressed in young people as compared to adults would not have been identified. It is likely that there may be, for example, safety behaviours or particular negative social cognitions that are specific to or more prevalent in younger people.
The participants recruited for this study were an analogue population of school children, rather than a clinical population, so the results may not be translatable to those who have been formally diagnosed with the condition. However, 33 (70.2%) of the participants from the high socially anxious group scored above the clinical cut-off recommended to indicate the presence of social phobia (Beidel et al., Reference Beidel, Turner and Fink1996). Their mean score on the SPAI-C was also 22.4, which is similar to the mean score of 24.6 obtained from a sample of young people who had been formally diagnosed with social phobia (Beidel et al., Reference Beidel, Turner and Fink1996). Thus some young people with clinical levels of social phobia may have been included in the sample. It seems important to replicate this study in a treatment-seeking clinical population to clarify whether the Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model is applicable to a clinical group of young people with social phobia. Additionally, as only 48% of the variance of social anxiety was explained by the cognitive model, it would be interesting to determine the extent to which other factors, such as parental anxiety, peer influence and family functioning predict childhood social anxiety. It would also be beneficial to examine the role of self-imagery and the use of internal cues to make inferences about how one appears, as these were components from the model that were not examined in this current study. Finally, the study could be developed if participants were followed over time, so that longitudinal data were obtained. There has been little investigation of the impact of the developmental trajectory on the aetiology or maintenance of social anxiety and future studies could help to elucidate this by using longitudinal designs. Nevertheless, Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) model is primarily concerning the maintenance of social phobia rather than the aetiology, and thus a cross-sectional study should be able to infer the applicability of the model to young people.
Given that Clark and Wells’ (Reference Clark, Butler, Fennell, Hackmann, McManus and Wells1995) cognitive model seems applicable for young people with social phobia, it would be interesting for further research to examine the effectiveness of a treatment package based on this theoretical framework for a younger population.
Acknowledgments
The authors are grateful to the Oxfordshire Education Authority for their support and would like to thank the Oxford Doctoral Course in Clinical Psychology for assistance in developing the study.




Comments
No Comments have been published for this article.