



Introduction
The recognition of the contribution of childhood circumstances to later-life health has important implications for the promotion of health among older people (Beard and Bloom, Reference Beard and Bloom2015), which currently focuses on behaviour changes in old age aimed at reducing the potential burden of an ageing population on health-care systems (Stephens, Reference Zimmer, Hanson and Smith2017). Lifecourse research from Europe and the United Kingdom (UK) has recently highlighted the impact of childhood socio-economic status (SES) on older-age health (e.g. Cosco et al., Reference Cosco, Hardy, Howe and Richards2018; Nurius et al., Reference Nurius, Fleming and Brindle2019). The recognition of the critical importance of the whole lifecourse is relatively new and as longitudinal studies provide lifecourse data, more evidence from other populations is needed to strengthen the message that societies must care for all people across the whole lifecourse to maintain health for all into older age (Walker, Reference Walker2013). In this paper we aim to test the European findings on a New Zealand sample. We additionally propose to test theoretical explanations (Lynch and Brown, Reference Lynch, Brown, Binstock and George2011) that the link between childhood SES and late-life physical, mental and social health is mediated by educational achievement and adult wealth accumulation, and that these pathways are moderated by gender and ethnicity.
Lifecourse approaches to ageing and health view old age as a phase of development that is the outcome of earlier influences (Moody, Reference Moody2006); they recognise the lifelong social, cultural and cohort influences on how people age (Hooyman, Reference Hooyman, Browne, Ray and Richardson2002). Lifecourse epidemiologists have recognised that health is not a static condition measurable at one point in time, but the result of a process of adaptation to changing circumstances (Kuh et al., Reference Kuh, Richards, Cooper, Hardy, Ben-Shlomo, Kuh, Cooper, Hardy, Richards and Ben-Shlomo2014) and that disparities in health in older age are the result of long-term cumulative disadvantage which begins in childhood (Shuey and Willson, Reference Shuey and Willson2008). Health from a lifecourse perspective depends on the available resources, life-long practices and experiences that are part of individual life histories.
Inequalities in access to resources across the lifespan shape the health and wellbeing of people as they age. Victor (Reference Victor2010) has demonstrated how differences in health in older age are related to social class, race, ethnicity, gender, education level, and material wealth or deprivation which produce lifelong inequalities. Chandola et al. (Reference Zimmer, Hanson and Smith2007) used longitudinal data to show that health disparities related to previous occupational status among older people persisted and increased with age. People from lower occupational grades who had poorer health were more likely to report a more rapid deterioration in physical health in early old age. Others have demonstrated the effects of adverse childhood experiences on mortality (Hayward and Gorman, Reference Hayward and Gorman2004), physical health (Nurius et al., Reference Nurius, Fleming and Brindle2019) and mental health (Cosco et al., Reference Cosco, Hardy, Howe and Richards2018) in adult life. Older people who have experienced a lifetime of deprivation are least likely to reach later life physically and financially able to maintain their own wellbeing. Critical gerontologists (e.g. Estes et al., Reference Estes, Biggs and Phillipson2003; Walker, Reference Walker, Cann and Dean2009) have focused on the broader structural influences of economic, political and social processes on the health of older people. They show how conditions experienced by particular demographic groups, such as those of different SES (Kok et al., Reference Kok, Aartsen, Deeg and Huisman2017), gender (Calasanti and Zajicek, Reference Calasanti and Zajicek1993) and ethnic groups (Jatrana and Blakely, Reference Jatrana and Blakely2008; Shuey and Willson, Reference Shuey and Willson2008), shape the health of people throughout life and are exacerbated in older age.
A weight of evidence now supports the link between SES and health (Hoffmann et al., Reference Hoffmann, Kröger and Pakpahan2018). Since the ‘Black Report’ (Townsend and Davidson, Reference Townsend and Davidson1982), international evidence has confirmed that health and mortality are related to material wealth and social status. Furthermore, this relationship is not simply the difference between poverty and wealth but is on a gradient in which the higher one's social status and income, the better the health outcomes (Wilkinson, Reference Wilkinson2005). Evidence to support the gradient relationship between SES and health has been reproduced using a number of different proxies for SES including income, material assets, education, parent's social class or area-level deprivation (Marmot, Reference Marmot2004). The relationship between SES and health has been understood in terms of material pathways and access to physical resources (Conger et al., Reference Conger, Conger and Martin2010; Kaikkonen et al., Reference Kaikkonen, Mikkilä, Magnussen, Juonala, Viikari and Raitakari2013; Ball, Reference Ball2015) or in terms of psychological resources such as life skills, resilience or sense of control (Marmot, Reference Marmot2004; Lynch and Brown, Reference Lynch, Brown, Binstock and George2011; Ferraro et al., Reference Ferraro, Schafer and Wilkinson2016). The impact of these material and non-material pathways may persist into adulthood, and then later life, continuing to influence health and functioning (Beck et al., Reference Beck, Franz, Xian, Vuoksimaa, Tu, Reynolds and Kremen2018; Moorman et al., Reference Moorman, Carr and Greenfield2018).
Inequalities are also amplified across the lifecourse. Unequal beginnings may give rise to even more unequal endings (Corna, Reference Corna2013), demonstrated by widening inequalities in old age (Crystal et al., Reference Crystal, Shea and Reyes2016). The cumulative advantage/disadvantage theory describes ‘the systemic tendency for interindividual divergence in a given characteristic (e.g., money, health, or status) with the passage of time’ (Dannefer, Reference Dannefer2003: S327), suggesting that circumstances in childhood shape subsequent experiences over the lifecourse, which consequently affect later-life outcomes (Lynch and Brown, Reference Lynch, Brown, Binstock and George2011). Low SES in childhood may impact later-life health indirectly by leading to different SES pathways through the lifecourse (Lynch and Brown, Reference Lynch, Brown, Binstock and George2011; Brandt et al., Reference Brandt, Deindl and Hank2012; Agahi et al., Reference Agahi, Shaw and Fors2014). SES in adulthood (reflected in education levels, occupation and wealth) is one key factor through which childhood SES impacts later-life health (Zhang et al., Reference Zhang, Hayward and Yu2016; Greenfield and Moorman, Reference Greenfield and Moorman2018). Evidence suggests that adult SES is shaped by childhood economic conditions and in turn shapes later-life health (Corna, Reference Corna2013; Zhang et al., Reference Zhang, Hayward and Yu2016; Zimmer et al., Reference Zimmer, Hanson and Smith2016). Beard and Bloom (Reference Beard and Bloom2015) drew on such findings to claim that, allowing for a genetic determination of 25 per cent of heterogeneity in health in older age, the remainder is the cumulative effect of lifelong health inequities.
It is also well established that health varies by gender. Women may live longer than men, but they have higher morbidity, lower quality of life and greater likelihood of functional limitations (Brown et al., Reference Brown, Richardson, Hargrove and Thomas2016). To understand these health disadvantages, Hooyman et al. (Reference Hooyman, Browne, Ray and Richardson2002) point out that discriminatory educational and employment opportunities and lower wages mean that women, particularly single mothers or minority group women, spend their life poorer than men. However, there are additional structural disadvantages including women's constrained choices, due to roles as family and community care-givers, which expose women to higher levels of stress (Gasper and van Staveren, Reference Gasper and van Staveren2003). Overall, as Calasanti (Reference Calasanti2007) has noted, these complex inequalities are continuous throughout the lifecourse. Many of the current cohort of older women have witnessed marked changes in gender roles in Western society over the last 80 years. In 1940, women were largely excluded from education and employment, and held significant care-giving responsibilities. Owing to ongoing shifts in women's roles, paid employment histories are more diverse between women than between men (Wahrendorf, Reference Wahrendorf2015), leading to differences in occupational class and retirement trajectories (Lahelma et al., Reference Lahelma, Pietiläinen, Chandola, Hyde, Rahkonen and Lallukka2019).
Ethnic group differences also illustrate how certain groups in a population systematically attain benefits over the lifecourse, which are translated into health advantages. Since the late 1960s, researchers have focused on health inequalities between ethnic groups (Lynch and Brown, Reference Lynch, Brown, Binstock and George2011) and there are marked disparities in health for indigenous and ethnic minority people around the world (Jones, Reference Jones2006; Jemal et al., Reference Jemal, Thun, Ward, Henley, Vilma and Murray2008; Bécares, Reference Bécares, Jivraj and Simpson2015). These patterns reflect the unequal distribution of resources and the exclusion experienced disproportionately by people with minority ethnic backgrounds (Karlsen et al., Reference Karlsen, Bécares, Roth, Craig, Atkin, Chattoo and Flynn2012) and Aotearoa/New Zealand provides a clear example of such stratification. There are persistent health inequalities between the indigenous Māori population and the majority non-Māori population (Woodward and Blakely, Reference Woodward and Blakely2014). Māori have lower life expectancy, while cardiovascular disease, cancer, respiratory disease and injury rates are higher among Māori (Anderson et al., Reference Anderson, Crengle, Kamaka, Chen, Palafox and Jackson-Pulver2006). Māori also face inequalities from the early stages of their educational and occupational career, are overrepresented in deprived geographical areas, are less likely to own their home and experience disparities in access to health care (Anderson et al., Reference Anderson, Crengle, Kamaka, Chen, Palafox and Jackson-Pulver2006; Ben et al., Reference Ben, Cormack, Harris and Paradies2017; Harris et al., Reference Harris, Cormack, Stanley, Curtis, Jones and Lacey2018). Colonisation of Aotearoa/New Zealand since the 18th century has been a major factor in creating this disparity through repression of Māori cultural practices, language and institutions, removal of the economic base of Māori society, and unequal access to social resources such as education and employment (Anderson et al., Reference Anderson, Crengle, Kamaka, Chen, Palafox and Jackson-Pulver2006). From around 1940, government policy towards Māori underwent a change towards social welfare strategies for the attainment of parity between Māori and non-Māori, while recognising cultural distinctiveness (Fleras, Reference Fleras1985). Although these changes were related to some reduction in Māori/non-Māori health inequalities, evidence shows that the differences have both widened and narrowed from the 1950s to 2006 owing to economic restructuring in the 1980s and health reforms in the 1990s (Tobias et al., Reference Tobias, Blakely, Matheson, Rasanathan and Atkinson2009). These shifts are ongoing and while such changes have occurred across the lifetime of older people, any health benefits may not be realised by older Māori today.
Lifecourse researchers (e.g. Stoller and Gibson, Reference Stoller, Gibson, Stoller and Gibson2000; Hinze et al., Reference Hinze, Lin and Andersson2012) have focused on the intersection of gender and ethnicity to show how disparities for minority ethnic group women have been related to physical and mental health disparities in older age. Intersectionality scholars argue that analysis of ethnic, gender and SES effects on health must take such interacting effects into account; however, few studies have examined how the interaction of these structural dimensions influences health across time (Brown, Reference Brown2018). Analysts using longitudinal data (e.g. Shuey and Willson, Reference Shuey and Willson2008; Brown et al., Reference Brown, Richardson, Hargrove and Thomas2016) have demonstrated interactions between ethnicity, gender, SES and education level in the effects of cumulative disadvantage on different health outcomes for older African and White Americans. However, there remains a lack of consensus regarding the ways in which these structural differences may moderate the effects of deprivation in early life on late-life health.
Healthy ageing outcomes are not well represented by physical health alone. Recent critiques, reviews and research including the views of older people themselves, agree on the need for inclusive and holistic definitions of good health in older age (Sadana et al., Reference Sadana, Blas, Budhwani, Koller and Paraje2016). These approaches emphasise that healthy ageing as a goal is broader than the absence of illness and more than maintaining physical functioning, because health includes psychological wellbeing and positive social relationships. These views are in accord with the World Health Organization (WHO) definition of health (included in the preamble to the Constitution of the WHO) which dates back to 1948: ‘Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity’ (WHO, Reference Zimmer, Hanson and Smith1948: 1). This multi-dimensional view, emphasising broader definitions of health, is particularly pertinent for studies of ageing, in which physical changes may be considered a normal part of ageing and should not be the sole focus of assessments of health (Marengoni et al., Reference Marengoni, Angleman, Melis, Mangialasche, Karp, Garmen, Meinow and Fratiglioni2011). Accordingly, health should be assessed in terms of physical, mental and social wellbeing as part of an ongoing developmental process.
Aims
Lifecourse research from Europe and the UK has highlighted the impact of SES pathways from childhood to older-age health. To test these international findings on a New Zealand sample we propose a model, in which the link between childhood SES and late-life physical, mental and social health is mediated by educational achievement and adult wealth accumulation as lifecourse aspects of SES (Figure 1). In addition, based on suggestions from research in the United States of America (USA), we propose that these pathways are moderated by gender and ethnicity. We hypothesise that:
(1) Childhood SES is related to physical, mental and social health across 10 years after the age of 60.
(2) The relationships between childhood SES and late-life physical, mental and social health are mediated by lifecourse SES pathways through educational achievement and mid-life adult wealth accumulation.
(3) Gender and ethnicity moderate these pathways.
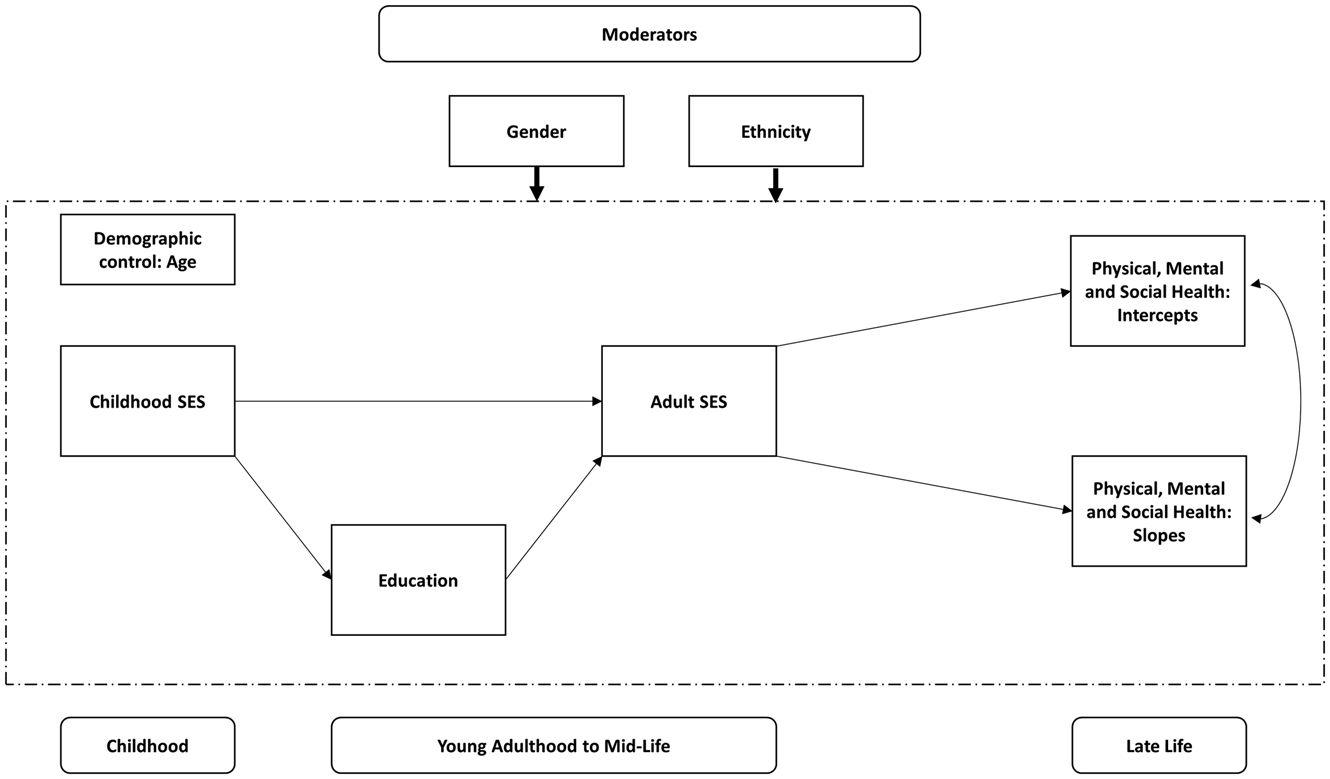
Figure 1. The proposed mediational model with gender and ethnicity as moderators.
Note: SES: socio-economic status.
Method
Data and sample
Data were collected between 2006 and 2016 as part of the Aotearoa/New Zealand Health, Work and Retirement Study (NZHWR). The NZHWR is a prospective cohort study that investigates social integration, economic wellbeing and health of New Zealanders aged 55 years and older. Data are collected biannually via postal surveys. In 2006, a random sample aged 55–70 years old was selected from the New Zealand electoral roll (N = 13,044; 4,769 from the general population and 8,275 from the Māori population). Persons of Māori descent were over-sampled to ensure adequate representation of the indigenous population in the study. A sample of N = 6,662 (46.5% Māori) returned the initial survey in 2006 resulting in a 51 per cent response rate. Of this sample, 46% (N = 3,065) agreed to be contacted for follow-up assessments every two years.
In 2017, additional Life Course History Interviews (LCH) were conducted to collect information on lifecourse determinants of health and wellbeing in later life. There were N = 1,133 eligible participants who entered the NZHWR in 2006 and were still active in the study in 2017. Of this sample, 804 consented and 787 were successfully interviewed. Structured interviews were conducted by trained interviewers using computer-assisted telephone interview software. Information was collected in 12 modules: demographic information; birth/adoption of children; partner history; accommodation history; childhood economic circumstances; employment history; financial history; childhood health history; adult health history; history of alcohol use; exposure to difficult or stressful life events; and periods of happiness and adversity. On average, the interviews took 1 hour and 45 minutes to complete.
The current sample included N = 729 participants (53% female, 40% Māori) who provided information on childhood economic circumstances, education, adult financial history, and late-life physical, mental and social health. The average age of the participants at the time of the interview was 72 years (standard deviation (SD) = 4.5 years; range = 61–81 years). The sample included 219 (30%) non-Māori men, 127 (17%) Māori men, 225 (31%) non-Māori women and 158 (22%) Māori women.
Variables
Late-life health
Information on physical, mental and social health in later life was collected from the longitudinal surveys between 2006 and 2016. The Short Form Health Survey (SF-12; Ware et al., Reference Ware, Keller and Kosinski1998) was administered to assess mental and physical aspects of health. The physical and mental health component scores of the SF-12 have been normed to the Aotearoa/New Zealand population using data from the New Zealand Health Survey (Frieling et al., Reference Zimmer, Hanson and Smith2013). Scores can range from 0 to 100, where 50 corresponds with the population average (SD = 10), and higher scores indicate better physical and mental health. Social health was measured with the Social Provisions Scale (SPS; Cutrona and Russell, Reference Cutrona and Russell1987), which assesses interpersonal relationships in six dimensions: attachment, social integration, reassurance of worth, reliable alliance, guidance and opportunity for nurturance. Items are rated on a four-point scale (1 = strongly disagree to 4 = strongly agree) and can be combined into a composite score (range = 24–96), where higher scores indicate greater relational provisions.
Socio-economic status
SES was assessed using a range of proxies which are most relevant for different stages of the lifecourse, including childhood living standards, educational level achieved, occupational grade and wealth in adult life.
Childhood SES
Childhood SES was assessed in terms of availability of socio-economic resources, main breadwinner's occupational grade, family literacy, housing quality and overcrowding at the age of 10. Availability of socio-economic resources included eight items from the New Zealand Material Wellbeing Index (Perry, Reference Perry2015), such as ‘Did you have suitable clothes for important or special occasions when you were 10?’ Responses to the main breadwinner's occupational grade were recoded into five levels based on the International Standard Classification of Occupations skill levels: no main breadwinner, elementary, skilled, associate and manager. The number of books available in the household was used as a proxy measure for family literacy. Response options included ‘none or very few (0–10 books)’, ‘enough to fill one shelf (11–25 books)’, ‘enough to fill one bookcase (26–100 books)’, ‘enough to fill two bookcases (101–200 books)’ and ‘enough to fill two or more bookcases (more than 200 books)’. Housing quality was determined based on the following features: fixed bath, cold running water supply, hot running water supply, inside toilet and heating supply. Overcrowding was calculated by dividing the number of people living in the household at the age of 10 by the number of rooms used as bedrooms in the house. This resulted in a scale that was recoded into ‘more than 1.5 people per room’ and ‘less than 1.5 people per room’. Principal component analysis (PCA) was used to create a relative measure of inequalities in childhood SES based on these indicators. The PCA indicated that all items loaded on the same latent dimension, which explained 41 per cent of the total variance. All loadings were above 0.35.
Education
Education was assessed as the highest level of educational qualification obtained. It was divided into four levels: no formal qualification, secondary qualification, post-secondary qualification and university degree.
Adult SES
Adult SES was measured as a combination of highest occupational grade and financial history. Occupational grade was defined as described above. Financial history included questions about investments (e.g. stocks, shares, property investments) and accumulation of assets (e.g. savings accounts, retirement accounts) measured with five items. In addition, participants were asked to indicate for each job throughout their lifecourse whether the income they earned met their everyday needs for necessities, such as food or accommodation. Responses were provided on a four-point scale: ‘not enough’, ‘just enough’, ‘enough’ and ‘more than enough’. Financial hardship was defined as the total number of periods when income was ‘not enough’ for everyday needs. PCA was employed to obtain a relative measure of inequalities in adult-life SES based on these indicators. The PCA indicated that all items loaded on the same latent dimension, which explained 40 per cent of the total variance. All loadings were above 0.40.
Data analysis
Preliminary analyses were performed in SPSS for sample description and to assess differences in the study variables across groups. All analyses distinguished between four groups: non-Māori men, Māori men, non-Māori women and Māori women.
We estimated changes in physical, mental and social health over a 10-year period of older adulthood using latent growth curve analysis (LGC) in Mplus (Muthén and Muthén, Reference Muthén and Muthén2017). LGC models have two main parameters: intercept and slope (Duncan and Duncan, Reference Zimmer, Hanson and Smith2009). In this case, the intercept refers to the average baseline score in 2006, and the slope indicates the average rate of change from 2006 to 2016. We modelled changes in physical, mental and social health simultaneously. After establishing change in the total sample, we performed a multi-group analysis to assess change trajectories based on ethnicity and gender.
Next, we performed a mediation analysis to assess the impact of childhood SES, education and adult-life SES on late-life health outcomes (Figure 1). We estimated the influence of lifecourse determinants on both the intercepts (i.e. baseline levels of physical, mental and social health in 2006) and the slopes (i.e. changes in physical, mental and social health from 2006 to 2016). The model included two mediator variables between childhood SES and late-life health: education and adult-life SES. Both direct and indirect effects were estimated. The analysis controlled for the influence of age on each path. After establishing the model for the total sample, multi-group analysis was performed based on gender and ethnicity.
Model fit was estimated using the following criteria: Comparative Fit Index (CFI) close to or greater than 0.95, Root Mean Square Error of Approximation (RMSEA) lower than 0.06 and Standardised Root Mean Square Residual lower than 0.08 indicating good fit to the data (Tabachnick and Fidell, Reference Tabachnick and Fidell2007). When comparing model fit obtained from the total sample with model fit from multi-group analyses, we relied on the CFI and RMSEA difference tests, with a reduction of 0.01 or less indicating invariance across groups (West et al., Reference West, Taylor, Wu and Hoyle2012). Missing data were handled with the full information maximum likelihood function (Geiser, Reference Geiser2013).
Results
Group comparisons
Significant differences were found between groups in childhood SES, adult-life SES and late-life social provisions (Table 1). Specifically, both non-Māori men and women reported significantly higher childhood SES than Māori men and women. Further, non-Māori men had significantly better adult-life SES than both Māori and non-Māori women. In terms of late-life social provisions, non-Māori women scored significantly higher than both Māori and non-Māori men.
Table 1. Differences across groups in study variables
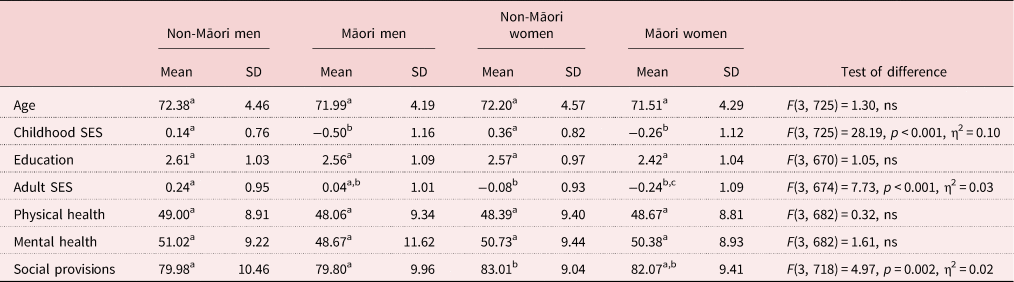
Notes: Tests are adjusted for pairwise comparisons using the Bonferroni correction. SD: standard deviation. SES: socio-economic status.
Significance levels: Values in the same row not sharing the same superscript letter are significantly different at p < 0.05. ns: not significant.
Changes in late-life health
In the total sample, the LGC analysis indicated that physical and social health declined from 2006 to 2016, whereas mental health remained stable over 10 years. Multi-group analysis indicated some variation in health trajectories across groups. Physical health declined across groups, with the decline being greater for Māori men and women. Mental health remained stable in all groups, except in Māori men who experienced improvements over time. With respect to social health, there was a small, significant decline in all groups, except in Māori men who remained stable over time. Model fit is reported in Table 2. Intercept and slope estimates for the total sample and by groups are reported in Table 3.
Table 2. Model fit

Notes: CFI: Comparative Fit Index. RMSEA: Root Mean Square Error of Approximation. CI: confidence interval. SRMR: Standardised Root Mean Square Residual.
Table 3. Changes in physical, mental and social health over 10 years in the total sample and by groups
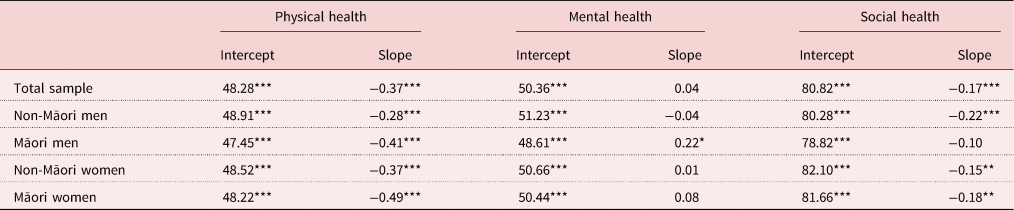
Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001.
Lifecourse determinants of late-life health
First, we estimated the mediational model for the total sample, which yielded a good fit to the data (Table 2). All standardised direct and indirect effects are reported in Table 4. Childhood SES was positively associated with the highest level of education obtained, which in turn was linked to greater adult-life SES. Childhood SES also had a direct effect on adult-life SES. Better adult-life SES predicted greater initial levels of physical and mental health in late life. Childhood SES had a direct positive effect on initial levels of mental and social health in late life. Similarly, education had a direct positive effect on initial levels of social health in late life. Childhood SES had positive indirect effects on initial levels of physical, mental and social health in late life through higher levels of education and higher adult-life SES. Education also had a positive indirect effect on initial levels of physical and mental health in late life via greater adult-life SES. None of the lifecourse variables had any influence on the slopes, i.e. the rate of change in health outcomes in late life.
Table 4. Standardised direct and indirect effects from the mediational model for the total sample and by groups
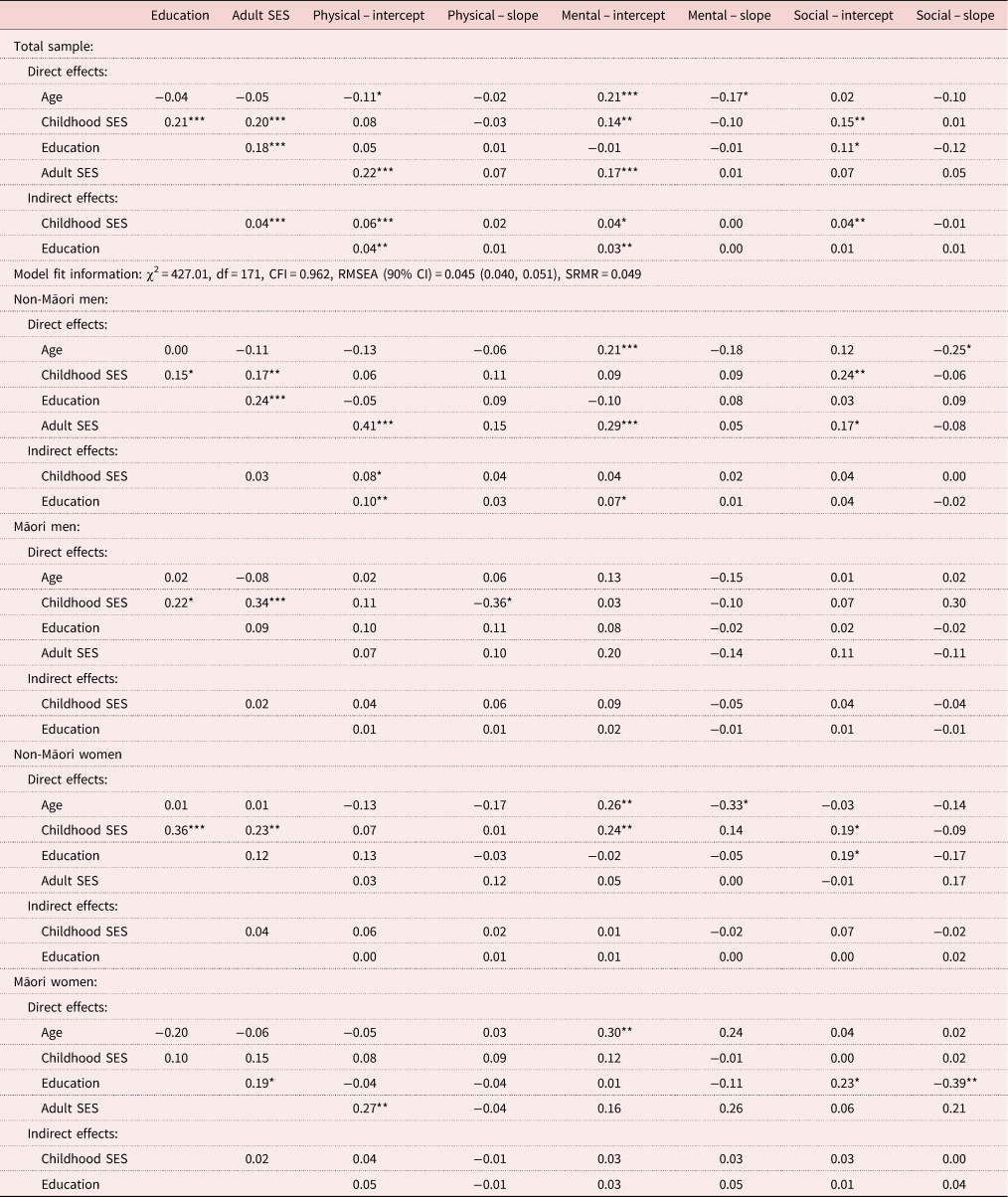
Notes: SES: socio-economic status. df: degrees of freedom. CFI: Comparative Fit Index. RMSEA: Root Mean Square Error of Approximation. CI: confidence interval. SRMR: Standardised Root Mean Square Residual. Multi-group analysis model fit information: χ2 = 1052.37, df = 680, CFI = 0.946, RMSEA [90%CI] = 0.055 [0.048; 0.061], SRMR = 0.076, ΔCFI = 0.016, ΔRMSEA = 0.010.
Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001.
Second, a multi-group analysis was performed to test the model across the four groups. While fit indices remained in the acceptable range, the overall fit of the model declined compared to the model fit obtained with the total sample, indicating variation across groups (Table 2).
The model with non-Māori men mirrored the results obtained with the overall sample. Childhood SES was positively associated with educational level, which in turn was associated with adult-life SES and leading on to initial levels of late-life physical, mental and social health. In addition, childhood SES had a direct positive effect on adult SES and an indirect effect on initial levels of late-life physical health via education and adult-life SES. Education also had positive indirect effects on initial levels of late-life physical and mental health through adult-life SES.
In the model with Māori men, childhood SES was predictive of levels of education and adult-life SES, but education was not significantly associated with adult-life SES. Further, adult-life SES was not significantly related to late-life health outcomes. However, childhood SES had a direct negative effect on the slope of late-life physical health.
Similarly, in non-Māori women, childhood SES was predictive of levels of education and adult SES, but education was not significantly associated with adult SES. Adult SES was also unrelated to late-life health outcomes. Childhood SES, however, had a positive direct effect on initial levels of late-life mental and social health. In addition, education had a direct positive effect on initial levels of late-life social health.
For Māori women, childhood SES was unrelated to education, adult-life SES and late-life health outcomes. Education, however, was positively associated with adult-life SES, which in turn predicted late-life physical health. Further, education significantly predicted both the intercept and the slope of late-life social health.
Discussion
The hypotheses were supported by the findings. First, childhood SES was an important predictor of later-life wellbeing for the whole sample. This finding adds to the results from European studies using data from the Survey of Health, Ageing and Retirement in Europe (SHARE) which have also demonstrated the effects of childhood SES on late-life health (Brandt et al., Reference Brandt, Deindl and Hank2012; Gruenewald et al., Reference Gruenewald, Karlamangla, Hu, Stein-Merkin, Crandall, Koretz and Seeman2012; Flores and Kalwij, Reference Flores and Kalwij2014; Mazzonna, Reference Mazzonna2014; Schaan, Reference Schaan2014). Our study provides additional support for recognition of the importance of childhood circumstances from another cultural context. A weight of evidence from a range of countries is required to reinforce the need for societies to support childhood wellbeing in order to support the future health of the whole population. The importance of this issue for social policy, as we grapple with the implications of an ageing population, is to shift attention from concerns with health improvement only in older age (when most of the damage has been done), to the effects of inequalities across the whole lifecourse.
The second contribution of these findings is to highlight the role of social structural mediators through which childhood SES maintains persistent effects across the lifecourse; the results support the second hypothesis predicting mediation effects through education and adult occupation and wealth. This supports previous findings that educational achievement mediates the effects of childhood SES on late-life cognition (Fritze et al., Reference Fritze, Doblhammer and van den Berg2014), health (Flores and Kalwij, Reference Flores and Kalwij2014) or depression (Schaan, Reference Schaan2014), and that adult employment situations can explain health in older age. Lower occupational grades with physically difficult work and lack of autonomy directly affect physical and mental health (Hämmig and Bauer, Reference Hämmig and Bauer2013; Wahrendorf et al., Reference Wahrendorf, Blane, Bartley, Dragano and Siegrist2013; Szabó et al., Reference Szabó, Allen, Stephens and Alpass2019). Lower-grade occupations also affect income and opportunities to accumulate wealth which is consistently related to health (van Doorslaer and Koolman, Reference van Doorslaer and Koolman2004). The evidence to date demonstrates the effects on late-life health of lifelong trajectories of unequal SES; inequalities in both childhood educational achievement and subsequent working conditions, and inequalities in income in adult life are all matters amenable to changes in social policy. For example, Mazzonna (Reference Mazzonna2014) compared lifecourse trajectories across different European countries (with different institutional and cultural environments) to show that country differences in education policies moderated the effect of childhood SES on health in older age. Schafer et al. (Reference Zimmer, Hanson and Smith2011) argue that real access to good-quality education regardless of family social position can equalise opportunities between individuals. Work and retirement policies can also address employment inequalities. Lahelma et al. (Reference Lahelma, Pietiläinen, Chandola, Hyde, Rahkonen and Lallukka2019) found that women who retired early due to disability had improved functioning over time compared to those who experienced mandatory retirement. This retirement trajectory went some way to addressing the health effects of lower occupational class among women. Corna (Reference Corna2013) has summarised work that recognises the effects of welfare state provisions on working-life experiences and subsequent health. The contribution of state provisions to health across the lifecourse deserves further scrutiny.
The key contribution of the current findings is support for the third, moderation, hypothesis. Our analysis demonstrated different pathways for different social groups which emphasises the importance of paying attention to diverse experiences; the average experience of the population does not necessarily reflect the experiences of different, especially marginalised, groups which may be obscured. A strength of our study is the use of data-set in which the Māori indigenous people, although a minority group in the population, were over-sampled to provide robust group comparisons. The different models pointed to important differences for Māori men and Māori and non-Māori women that do not reflect our whole-sample findings, nor the European findings cited above. The patterns of relationships in our findings suggest that gender and ethnicity are associated with different lifetime education, employment and SES trajectories that deserve further longitudinal investigation. These findings show important differences to the general model that was based on theoretical and empirical work conducted in Europe and the USA, and highlight the need to consider cultural and group differences, and their intersections, in different contexts (Read and Gorman, Reference Read and Gorman2006; Hinze et al., Reference Hinze, Lin and Andersson2012; Corna, Reference Corna2013).
The lifecourse factors of childhood and adult SES explained health around the time of entry to older age for most groups. This finding suggests that the lifecourse is an important determinant of levels of physical, social and mental health with which people arrive at older age. Improvements in lifecourse determinants, including childhood advantage, can support people to traverse older age with optimum levels of health and wellbeing. However, the ability to enjoy sustained lifetime health benefits from these improvements in childhood advantages does depend upon gender and ethnicity.
These findings point to the need to consider lifelong impacts on health in older age, and the importance of recognising how the diverse experiences of different socially structured groups produce different pathways to health. There are several limitations in the current study which should be addressed in future research. Māori men and women reported significantly lower levels of childhood SES using the present measures. This may well reflect poorer childhood circumstances for Māori, but the measures used require further validity testing for these groups. In general, there are cultural differences in Māori social life that may not be well explained by the constructs and measures used in this study. Further validation work with local populations is required. The present sample also included a relatively advantaged group of healthy survivors, which will, however, only attenuate the strength of the association between SES and health outcomes.
Conclusion
Two key messages are supported by our findings. First, is the importance of the lifecourse in producing and reinforcing health inequities in older age. Societal action across the lifecourse, beginning in childhood and continuing through education and adult life, rather than individually focused education and intervention aimed specifically at older people, is needed to create a social environment that supports and maintains good health at all stages of life. The second key issue is the diversity of ageing experiences and the need to include more nuanced understandings of different health trajectories in older age. Attention to diversity will enable the recognition of the breadth and impact of inequalities on the health of current cohorts of elders, so that their damaging effects are not reinforced by present policies and practices which expect every older person to strive to achieve ‘successful ageing’ (Stephens and Breheny, Reference Stephens and Breheny2018). Policies that foster broad-based interventions such as raising retirement age, or encouraging volunteering to improve health, place many older people in demanding situations that only exacerbate their health issues (Ranzijn, Reference Zimmer, Hanson and Smith2010; Walker, Reference Walker2013; Beard and Bloom, Reference Beard and Bloom2015; Stephens et al., Reference Zimmer, Hanson and Smith2015). The public health responses to issues around the health of older people must include recognition of diverse health pathways, the social circumstances that affect late-life wellbeing and the effects of life-long inequalities.
Author contribution
CS developed the conceptual background and drafted the introduction and discussion. ÁS conducted the data analysis and wrote the method and results. MB collected the data. All authors contributed to the development, analytic framework, writing and final form of the paper.
Financial support
The longitudinal study was supported by successive grants from the Health Research Council of New Zealand (05/311); Foundation for Research and Technology, New Zealand (MAUX0401); and Ministry of Business, Innovation and Employment, New Zealand (MAUX1205, MAUX1403).
Ethical standards
Ethics approval for all data collection waves in this study were granted by Massey University Human Ethics Committee (MUHEC). Approval was granted under the following protocols: MUHEC Southern A – 05/90: ‘A study of the health of older adults in the transition from work to retirement’ (2006–2008); MUHEC Southern B – 09/70: ‘Postal surveys for the New Zealand Longitudinal Study of Ageing’ (2010–2012); MUHEC Southern A – 15/72: ‘Health, work and retirement survey 2016–2018’ (2016–2018); a low risk notification was provided to MUHEC in 2014; MUHEC Southern A – 15/45: ‘Health, work and retirement life history interview’ (2015–2017).
Conflict of interest
The authors declare no conflicts of interest.





