



Introduction
In recent decades, a growing body of literature links social capital and built environment with the mental health of elderly people. Social capital and the built environment significantly influence the psychological wellbeing of elderly people. Although the above relationship in western countries has been repeatedly discussed, in countries in the developing world, such as China, it has rarely been examined. The research associated with China includes only a few studies that explore the relationship between social capital and health outcomes (Norstrand and Xu, Reference Norstrand and Xu2012) and between the built environment and the quality of life among elderly people (Liu et al., Reference Liu, Dijst, Faber, Geertman and Cui2017; Feng et al., Reference Feng, Tang and Chuai2018). As the pace of ageing is the most rapid and the size of the elderly population is the largest in the world, there exists a need to examine the interconnection among social capital, built environment and mental health among the elderly people in China (England, Reference England2005; National Bureau of Statistics of the People's Republic of China, 2017).
Owing to rapid urbanisation, elderly migrants in urban China have reached a sizeable number. In contrast to western countries, a considerable share of the elderly migrants float to cities where their sons or daughters live in order to care for their children and grandchildren, probably because ‘family values’ are highly emphasised in traditional Chinese culture (Fei, Reference Fei1983) and family support from parents is still prevalent in contemporary China (Sun and Wang, Reference Sun and Wang2010). Compared to the local elderly people, this group of elders (the so-called ‘laopiao’), who cut off their social networks in their hometowns and leave their familiar environment, has distinctive characteristics and is often believed to have poorer mental health than local elderly people (Liu, Reference Liu2016). Nevertheless, previous studies tend to treat all of the elderly people in urban China as an entirety. The differences in mental health between the local elderly people and the laopiao and whether such differences are determined by social capital and the built environment are questions that remain unanswered. Moreover, examining the effects of social capital and the built environment on the mental health of these two groups of elderly people can provide policy makers with valuable information to cater to different groups of elderly people.
Socio-economic and cultural circumstances in China are unique, which provides an ideal setting to explore the determinants of mental health among elderly people. Compared to western countries, China has experienced an unprecedented transition in social structure, physical environment and culture. Unlike many developing countries, China embraces a fast-growing number of elderly people in cities and a distinctive social context (i.e. family systems and social relations are grounded on Confucianism). Hence, the effects of social capital and the built environment on the mental health of elderly people in China may be different from their western counterparts.
Therefore, this study seeks to address the following research questions systematically:
(1) What is the inter-relationship among social capital, the built environment and mental health among elderly people in Chinese settings?
(2) What are the disparities between the local elderly people and the laopiao in urban China in terms of the effects of social capital and built environment on mental health?
The associated findings not only benefit Chinese elderly people (especially laopiao), who account for a large share of the total population in China, but also offer insights into the determining factors of mental wellbeing among elderly people in a transitional socio-economic setting with unique cultural accumulations. Our analysis is grounded on a survey conducted in Nanjing in 2015. This paper is structured as follows: the next section reviews the relevant literature, then an overview of the data and research area is presented. After proposing our conceptual model in the following section, the inter-relationships among social capital, the built environment and the mental health of local elderly people and the laopiao are analysed. The implications of our findings are discussed in the concluding section.
Literature review
Social capital and mental health
Several studies demonstrate that social capital is related to mental wellbeing, whether social capital lies in social networks and social support at the individual level (Portes, Reference Portes1998; Coleman, Reference Coleman1990) or works through a mechanism by social participation and reciprocity at the collective level (Putnam et al., Reference Putnam, Leonardi and Nonetti1993). Generally, narrower social networks and inadequate social support are associated with negative mental health (Barnett and Gotlib, Reference Barnett and Gotlib1985), while cognitive social capital such as trust and security contributes to people's mental health. For instance, trust has a positive effect on the psychological health of the population in rural China through the pathways of social networks and support (Yip et al., Reference Yip, Subramanian, Mitchell, Lee, Wang and Kawachi2007), while a diminished sense of trust in people is a factor of poor mental health in Colombia (Harpham et al., Reference Harpham, Grant and Rodriguez2004). A similar result is found in Britain: general trust is positively associated with the psychological health of the population (Giordano and Lindström, Reference Giordano and Lindström2011). In addition to trust, a sense of security is linked to mental health among people in Finland (Nyqvist et al., Reference Nyqvist, Finnas, Jakobsson, Jakobsson and Koskinen2008).
Despite the growing body of literature on the relationship between social capital and mental health, research focusing on elderly people is relatively scarce. Several indicators of social capital, such as trust, social integration and social participation, have been employed to investigate the mental wellbeing of elderly people in previous studies. At the individual level, social networks and social support from families, friends or neighbours play an important role in the mental health of elderly people. It is observed that not being married or co-habiting is correlated with depressive symptoms in South Africa (Ramlagan et al., Reference Ramlagan, Peltzer and Phaswana-Mafuya2013). Having friend networks is shown to help decrease the level of depressive symptoms of older Americans (Litwin, Reference Litwin2011). Also, social contacts with family members, friends or neighbours improve psychological health in Sweden (Nyqvist et al., Reference Nyqvist, Gustavsson and Gustafson2006). Difficult access to instrumental social support from neighbours shows a significant association with depression among elderly people in Finland (Forsman et al., Reference Forsman, Nyqvist and Wahlbeck2011). At the collective level, Nyqvist et al. (Reference Nyqvist, Gustavsson and Gustafson2006) found a negative association between social participation and psychological health of elderly people, whereas depression among European elderly people became less severe when their social participation increased (Abu-Rayya, Reference Abu-Rayya2006). This is because diverse social networks can improve the level of mental health (Litwin, Reference Litwin2011), while civic engagement is related to good cognitive functioning among elderly people (Ramlagan et al., Reference Ramlagan, Peltzer and Phaswana-Mafuya2013).
In addition to the investigation of the relationship between social capital and the mental health of elderly people at the individual and collective levels, a handful of empirical studies have decoupled social capital into bonding, bridging and linking capital, with their respective effects on the mental wellbeing of elderly people differentiated. Bonding social capital is derived from ‘inward-looking’ social relationships among persons with similar characteristics (such as age, education and ethnicity); bridging social capital is based on ‘outward-looking’ connections among heterogeneous people at the same level of hierarchy (Szreter and Woolcock, Reference Szreter and Woolcock2004); and linking social capital highlights the social networks between individuals and groups across the levels of hierarchy and power (Ferlander, Reference Ferlander2007). Adopting such classification, Norstrand and Xu (Reference Norstrand and Xu2012) found that bonding social capital is related to the emotional health of elderly people in urban China. Also, it is observed that both bonding and bridging social capital improve the mental health of Japanese elderly people (Murayama et al., Reference Murayama, Nishi, Matsuo, Nofuji, Shimizu, Taniguchi, Fujiwara and Shinkai2013).
In the existing literature, relevant research concerning China is very scarce; only two studies can be found. The first explores the relationship between social capital and quality of life among elderly people in Shanghai (Chen et al., Reference Chen, Wong and Chan2009), and the second examines social capital and its relationship with emotional health among Chinese elderly people along the urban–rural dimension (Norstrand and Xu, Reference Norstrand and Xu2012). Compared to the findings in western settings, social capital with Chinese features bears a different relationship to mental health among Chinese elderly people. In China, organisation-based social capital is less prevalent than in western countries (Norstrand and Xu, Reference Norstrand and Xu2012), while Chinese culture treats the family as a strong social unit (Bian et al., Reference Bian, Logan and Bian1998). Guanxi, which refers to the personal network featuring particularistic and reciprocal ties (Jacobs, Reference Jacobs1979), plays a vital role in Chinese societies. For instance, it is observed that bonding capital, rather than western-oriented formal member organisation-based social capital, is significantly associated with better emotional health among elderly people in China (Norstrand and Xu, Reference Norstrand and Xu2012).
Built environment and mental health
The built environment is a broad term, encompassing dwellings, spaces and other aspects of habitat that are created or modified by people (Clarke et al., Reference Clarke, Ailshire, Bader, Morenoff and House2008). In recent decades, the relationship between the built environment and the general health of the population (such as obesity, physical activities and mental illness) has been widely investigated. There is growing evidence showing that the built environment has a significant effect on people's mental health. For instance, dwelling characteristics such as physical housing quality and housing structure are associated with individual mental health (Evans et al., Reference Evans, Wells, Chan and Saltzman2000; Weich et al., Reference Weich, Blanchard, Prince, Burton, Erens and Sproston2002). At the neighbourhood level, the good features of the built environment, such as quality sidewalks and green spaces, improve psychological wellbeing (Dalgard and Tambs, Reference Dalgard and Tambs1997; Galea et al., Reference Galea, Ahern, Rudenstine, Wallace and Vlahov2005; Araya et al., Reference Araya, Montgomery, Rojas, Fritsch, Solis, Signorelli and Lewis2007), whereas poor neighbourhood conditions and neighbourhood disorder, such as lack of recreation space or private gardens, poor street conditions and high crime levels, harm mental health (Latkin and Curry, Reference Latkin and Curry2003; Kearns et al., Reference Kearns, Whitley, Bond and Tannahill2012). In addition, the inter-relationship among accessibility to public facilities and open spaces, land-use mix, urban structure, residential density and mental health have been studied (de Vries et al., Reference de Vries, Verheij, Groenewegen and Spreeuwenberg2003; Caldwell et al., Reference Caldwell, Jorm and Dear2004; Melis et al., Reference Melis, Gelormino, Marra, Ferracin and Costa2015).
Nonetheless, the primary concern of the above studies is the health of the adult population, while the effect of the built environment on mental wellbeing among elderly people, who are more likely to have a high level of morbidity, mortality and disability, has been examined rarely (Garin et al., Reference Garin, Olaya, Miret, Ayuso-Mateos, Power, Bucciarelli and Haro2014). According to the limited pieces of literature, mental health among elderly people, especially the symptoms of depression, is linked to the type and quality of housing and perception towards their housing at the household level (Chan et al., Reference Chan, Malhotra, Malhotra and Ostbye2011; Lai and Guo, Reference Lai and Guo2011), as well as land use, open space and facility availability at the neighbourhood level (Berke et al., Reference Berke, Gottlieb, Moudon and Larson2007; Saarloos et al., Reference Saarloos, Alfonso, Giles-Corti, Middleton and Almeida2011). At the dwelling level, housing quality is positively related to the psychological wellbeing of elderly Americans (Evans et al., Reference Evans, Kantrowitz and Eshelman2002); living in a terraced dwelling can reduce the mental distress of older men in the United Kingdom (UK) (Sarkar et al., Reference Sarkar, Gallacher and Webster2013).
In addition to research regarding the features at the dwelling level, other studies have paid attention to the features at the neighbourhood level. It has been demonstrated that a higher degree of the land-use mix is associated with the negative mental health of older people (Saarloos et al., Reference Saarloos, Alfonso, Giles-Corti, Middleton and Almeida2011; Sarkar et al., Reference Sarkar, Gallacher and Webster2013). The accessibility to facilities has an effect on the emotional wellbeing of elderly people. For instance, retail availability is related to higher odds of depression for older men in Western Australia (Saarloos et al., Reference Saarloos, Alfonso, Giles-Corti, Middleton and Almeida2011). A higher degree of street network accessibility can alleviate the mental problems of older men in the UK (Sarkar et al., Reference Sarkar, Gallacher and Webster2013). Recreational facilities play an important role in older people's psychological wellbeing in Hong Kong (Phillips et al., Reference Phillips, Siu, Yeh and Cheng2005). Also, accessibility to transport facilities (such as subways and roads) and neighbourhood walkability affect the mental health of older men (Phillips et al., Reference Phillips, Siu, Yeh and Cheng2005; Berke et al., Reference Berke, Gottlieb, Moudon and Larson2007). In addition, it is observed that green areas or parks have an effect on the mental health of elderly people (Phillips et al., Reference Phillips, Siu, Yeh and Cheng2005; Parra et al., Reference Parra, Gomez, Sarmiento, Buchner, Brownson, Schimd, Gomez and Lobelo2010). Outdoor open space promotes the mental health of elderly people through social interaction and physical activity (Sugiyama and Thompson, Reference Sugiyama and Thompson2007).
In contrast to the sizeable amount of studies in western countries, very few studies assessed the influence of the built environment on emotional wellbeing among elderly people in mainland China. Similar to the findings in other regions or countries, it is observed that the quality of housing and neighbourhood environment is associated with the psychological wellbeing of elderly people (Lai and Guo, Reference Lai and Guo2011; Yan et al., Reference Yan, Gao and Lyon2014; Liu et al., Reference Liu, Dijst, Faber, Geertman and Cui2017; Feng et al., Reference Feng, Tang and Chuai2018). Despite the limited research concerning China, evidence shows that China's unique built environment has a significant effect on the wellbeing of elderly people. Since the economic reform of the late 1970s, China has undergone a dramatic transition, resulting in diverse living environments in urban areas. A work-unit (danwei) community built in the pre-reform period is characterised by a gated residential block, which is significantly different from those in the commercial housing communities that flourished after the reform. Also, traditional neighbourhoods in cities are often surrounded by modern districts with differential street density and distribution of facilities. The typical built environment in urban China might exert a unique impact on mental health in those areas. In the existing research, Yan et al. (Reference Yan, Gao and Lyon2014) divided neighbourhoods in Beijing into four types. It is found that neighbourhood environment and senior services display an important role in the life satisfaction of elderly people in the old mixed community and the work-unit community of Beijing (Yan et al., Reference Yan, Gao and Lyon2014). Feng et al. (Reference Feng, Tang and Chuai2018) demonstrated that some factors (informal space and work-unit community) that have Chinese features are negatively associated with the quality of life of older people. In addition, different from some findings in developed countries, population density has no significant effect on the quality of life of elderly people, revealing the disparities in the influence of urban form in different socio-economic contexts (Feng et al., Reference Feng, Tang and Chuai2018).
Local elderly people and laopiao in urban China
In China, urban elders can be divided into two distinctive groups: local elderly people and the laopiao. Laopiao represents the elder migrants who float from their origins to cities where their sons or daughters live to care for their children and grandchildren. In contrast to western settings, the laopiao account for a considerable share of the total elders in Chinese cities, especially in large cities. That is because ‘family values’ are highly emphasised in traditional Chinese culture (Fei, Reference Fei1983). Even in contemporary China, family support from parents still plays a prominent role in people's daily lives (Sun and Wang, Reference Sun and Wang2010). Also, alongside the rapid process of urbanisation in China, many youths move to other cities to work and live rather than remain in their hometowns, thereby increasing the number of the laopiao.
The laopiao have some distinct characteristics. Compared to local elderly people, the laopiao are more likely to co-reside with their children, and have more difficulties adapting to the living environment. Moreover, they tend to have more domestic and child-care work, but have fewer out-of-home leisure activities and fewer chances of interacting with other urban residents outside family networks. Hence, the laopiao, who cut off their social networks in their hometowns and leave their familiar environment, are reported to have poor mental health (Liu, Reference Liu2016).
Based on our literature review, we found that research about the connections among social capital, built environment and mental health of elderly people is very scarce. The majority of the studies on this topic focus on the mental health of elderly people in western countries, while studies of Chinese elderly people, who are quite different from their western counterparts, have rarely been touched on. Furthermore, those studies treat different groups of elderly people as an entirety, while the differences between various types of elderly people remain unknown. Thus, the following research questions are raised in this study:
(1) What is the inter-relationship among social capital, built environment and mental health of elderly people in the Chinese settings?
(2) What are the disparities between local elderly people and the laopiao in urban China in terms of the effects of social capital and built environment on mental health?
Data and method
Data source and study area
According to the law of the People's Republic of China on the protection of the rights and interests of elderly people, elderly people in China are defined as those aged 60 years and above, which follows the standard in many western countries. Therefore, the survey used in the paper adopts the definition in the law, focusing on people aged 60 years and above (elderly people in China). The survey, conducted between September and November 2015, concerns the living conditions of elderly people in urban Nanjing. Nanjing was chosen as the research area because it is located in the affluent eastern coastal region of China. Also, Nanjing is the capital city of Jiangsu and the sub-centre of the Yangtze Delta after Shanghai. The per capita Gross Domestic Product of Nanjing is ranked the top among the municipalities and prefecture-level cities across China. Due to the high development level, Nanjing attracts a massive number of migrants. In 2015, Nanjing administered a total population of 8.23 million, of whom 1.72 million were migrants (Jiangsu Provincial Bureau of Statistics, 2016). Of those migrants, the laopiao who follow their migrant children have accounted for a prominent share.
Our survey employed a stratified sampling method. Based on the built environment associated with the location and the interior and exterior environments of the communities, 12 representative communities were selected in the entire Nanjing metropolitan region (see Figure 1 and Table 1). In our sampling procedure, prior knowledge was adopted, which can produce better strata efficiency than systematic sampling or random sampling. In addition, it makes the variance within the strata smaller than within the overall population (Yan et al., Reference Yan, Gao and Lyon2014). In the survey, the distance between the community and the city centre, the type of community (danwei community/commercial housing community/affordable housing community) and the facilities nearby (e.g. metro station, park, supermarkets and gyms) were taken into account. In each of the selected communities, around 50 elderly respondents were sampled randomly. We surveyed the respondents face-to-face in their communities or at their homes. A total of 650 questionnaires were collected in the survey. Excluding those elderly who floated to Nanjing for reasons other than looking after their children and grandchildren, 591 respondents (412 local elderly people and 179 laopiao) were included in this study.
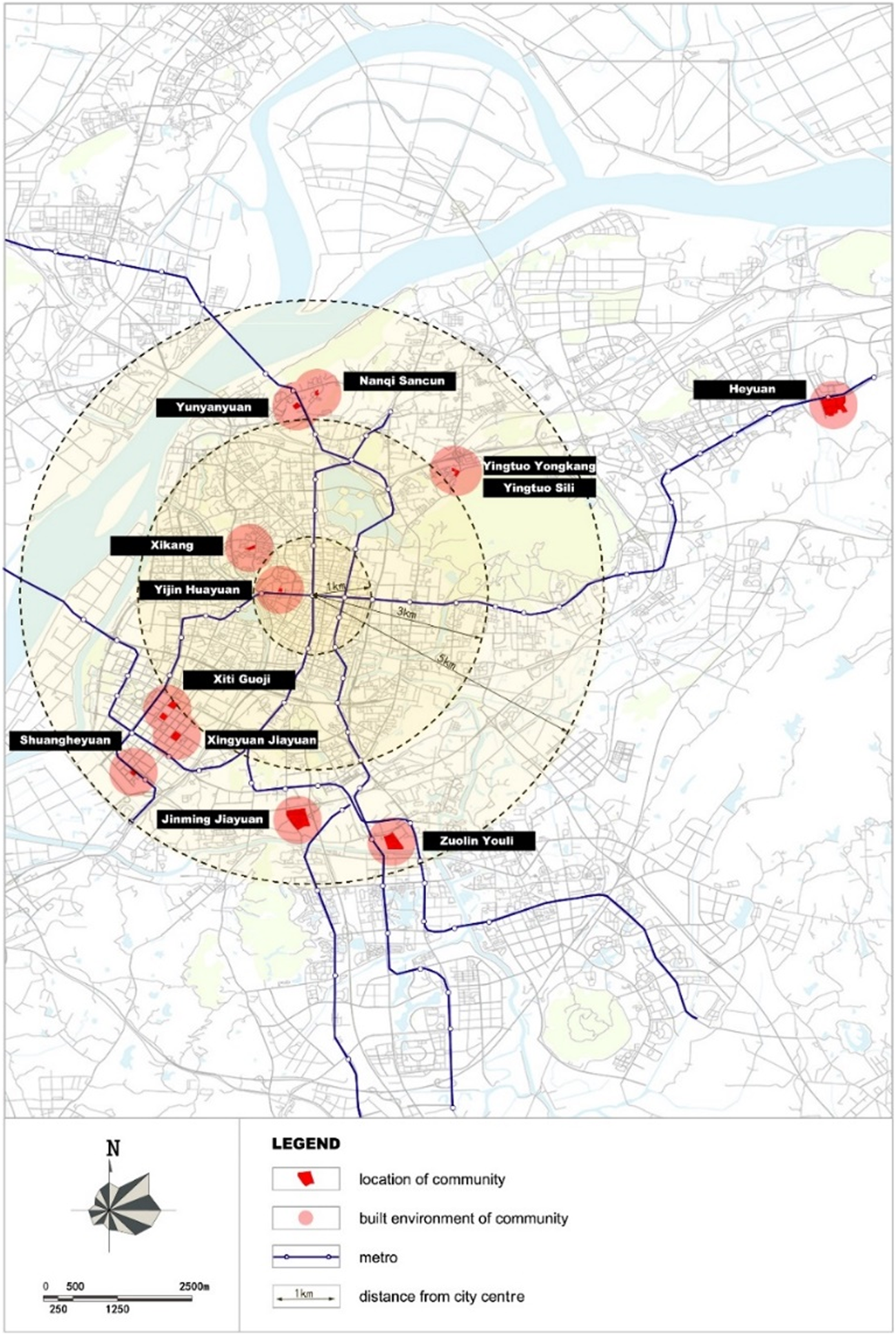
Figure 1. Locations of the 12 communities in Nanjing.
Table 1. Built environments of the 12 communities in Nanjing
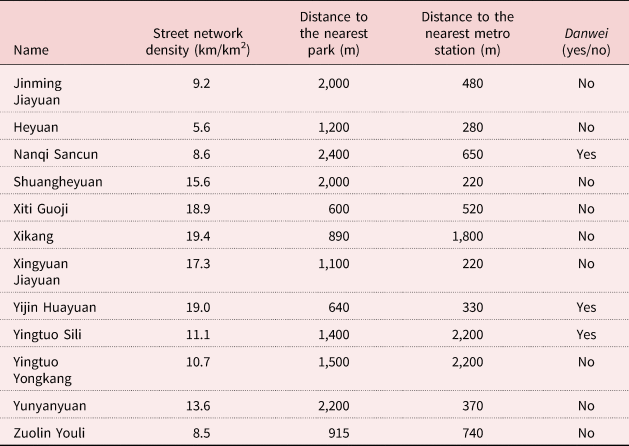
Notes: km: kilometre. m: metre.
Before exploring the inter-relationship among social capital, the built environment and the mental health of the elderly people in urban China, we have measured the construct validity and reliability of items used in the model by using SPSS 22.0. The score of Bartlett's test is less than 0.05, and the score of Kaiser–Meyer–Olkin (KMO) is 0.774. Moreover, the value of Cronbach's alpha is 0.767. Those scores indicate that the validity and reliability of our questionnaire items are good.
Conceptual framework
Based on existing literature, a conceptual framework was developed to investigate the association between social capital, built environment and mental wellbeing among Chinese elderly people (Figure 2). In the model, self-reported mental health was defined as the dependent variable, which is related to the factors of social capital, built environment and socio-economic status. Among the factors, those concerning social capital were selected as the endogenous variables, while the built environment and socio-economic status are considered as the exogenous variables. In other words, social capital, which is affected by objective built environment and socio-economic status, influences the self-reported mental health of elderly people. Previous studies argued that the mental health of elderly people is affected by ‘inward-looking’ social capital at the individual level and ‘outward-looking’ social capital at the collective level. In reference to previous studies (Norstrand and Xu, Reference Norstrand and Xu2012; Murayama et al., Reference Murayama, Nishi, Matsuo, Nofuji, Shimizu, Taniguchi, Fujiwara and Shinkai2013), we classified social capital in the model into three categories: bonding capital, bridging capital and linking capital. Specifically, bonding capital concerns the social networks of family members, friends and neighbours. Bridging capital assesses the relations at the organisation or community levels. Linking capital is based on the social networks across the levels of hierarchy and power, involving the Communist Party and public institutions in the model. The three categories of factors can capture the social capital of elderly people holistically.
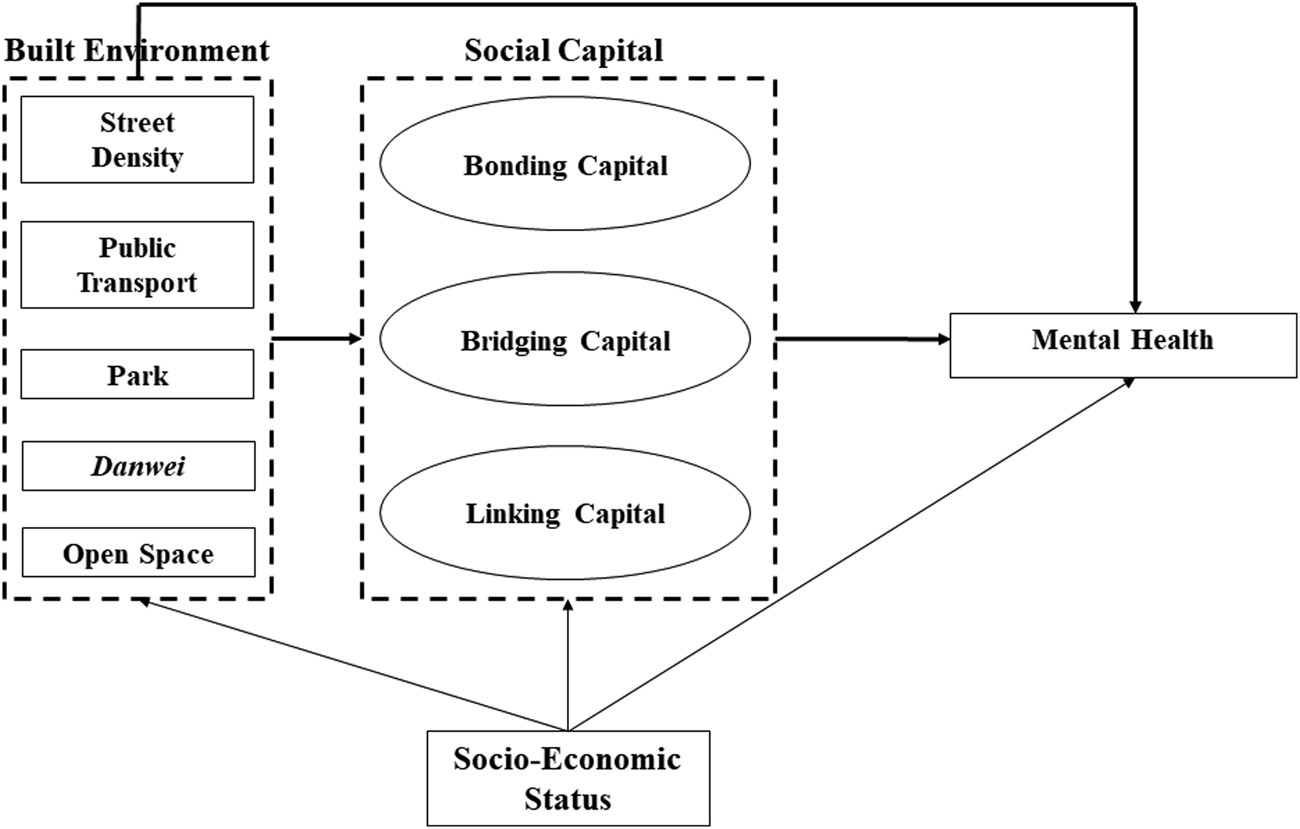
Figure 2. Conceptual framework.
In the model, the built environment includes five components, including street network density, accessibility to public transport, accessibility to parks, danwei and open space within a community. The selection of the built environment factors is made in reference to previous studies (Phillips et al., Reference Phillips, Siu, Yeh and Cheng2005; Parra et al., Reference Parra, Gomez, Sarmiento, Buchner, Brownson, Schimd, Gomez and Lobelo2010; Saarloos et al., Reference Saarloos, Alfonso, Giles-Corti, Middleton and Almeida2011; Sarkar et al., Reference Sarkar, Gallacher and Webster2013), which explore, respectively, the four representative aspects of the built environment: density, facility accessibility, open or green spaces, and type of community. In the model, the socio-economic factors of the respondents, including basic socio-demographics (age, gender and marital status) and socio-economic status, are included as control factors. The selection of the socio-economic factors is made according to prior studies regarding the health of elderly people in China (Yan et al., Reference Yan, Gao and Lyon2014; Liu et al., Reference Liu, Dijst, Faber, Geertman and Cui2017; Feng et al., Reference Feng, Tang and Chuai2018). Those variables are proven as factors that influence the health of elderly people in urban China. In addition to the factors adopted in research in western settings, additional factors such as membership of the Communist Party and work-unit community are also included in the model to capture the Chinese context better. The specific reasons for selecting those variables in the model are described in the following section.
In the study, structural equation models were adopted to identify the causal relationships between social capital, built environment and mental health. Structural equation modelling is a method combining regression, factor and path analyses together, which measures the relationships between the observed and the latent variables and the relationship among the latent variables (Bielby and Hauser, Reference Bielby and Hauser1977).
Mental health
Self-reported mental health was measured on a five-point Likert scale on which respondents rated their mental health as very poor (1), poor (2), fair (3), good (4) and very good (5). Previous studies showed that self-reported health is a general health status indicator predicting mortality, over and beyond the ‘objective’ measures of health status and other relevant covariates known to predict mortality (Idler and Benyamini, Reference Idler and Benyamini1997).
Social capital
Bonding capital
The perception towards homogenous networks, including family, friends and neighbourhood, was examined based on six questions in the survey. First, the capital of personal networks (family and friends) was investigated by presenting the participants with the following statements: ‘I am satisfied with my family relationship’, ‘I rely on family members when encountering problems’, ‘I share happiness and sadness with friends’ and ‘I rely on friends when encountering difficulties’. Second, social network in the neighbourhood was regarded as a perceptive relationship with neighbours. This concept was examined through two statements: ‘I chat with neighbours’ and ‘I and my neighbours help each other’. For each statement, respondents rated on a five-point ordinal scale (1 = disagree, 2 = slightly disagree, 3 = fair, 4 = slightly agree, 5 = agree). ‘Agree’ means that participants thought they have a better relationship with people who have similar social characteristics; whereas ‘disagree’ means that they thought they have poor social networks.
Bridging capital
Bridging capital was assessed by ‘outward-looking’ social networks across different groups who do not need to hold similar social characteristics (Murayama et al., Reference Murayama, Nishi, Matsuo, Nofuji, Shimizu, Taniguchi, Fujiwara and Shinkai2013). To distinguish the laopiao from the local elderly people, two indicators were adopted to reflect their network heterogeneity based on the following questions: ‘How many social groups or organisations do you participate in?’ and ‘Do you participate in community activities or not?’ (1 = yes, 2 = no). For the first question, if the respondents participate in more social groups and organisations, it implies that they have more heterogeneous networks. For the second question, the response of ‘yes’ means that the respondents may have more social networks with residents who are different from them, whereas ‘no’ indicates that the respondents tend to have smaller social networks.
Linking capital
Two indicators were used to measure the linking capital of the respondents, which come from two questions in the survey: ‘Are you a member of the Communist Party of China?’ and ‘Are/were you a cadre of government or a public institution of China?’ In China, the Communist Party and the government have a dominating social and political power (Norstrand and Xu, Reference Norstrand and Xu2012). The members of the Communist Party and the administrative staff of the government or public institutions are usually powerful elites in a high position in the social hierarchy.
Built environment
Street network density
Street network density is a useful indicator of the patterns of the neighbourhood environment. It plays an essential part in public health (Marshall et al., Reference Marshall, Piatkowski and Garrick2014). In this study, street network density was calculated by the length of the arterial and collector roads within a one-kilometre street network buffer of a surveyed community.
Accessibility to public transport or a public park
Accessibility to public transport or a public park was measured by the distance between the entrance of the surveyed community and the nearest metro station or public park. The previous study indicated that those facilities could help elderly people to benefit from physical activities and contact with nature and people and, hence, improve their mental wellbeing (Sugiyama and Thompson, Reference Sugiyama and Thompson2007).
Danwei community
Danwei community was measured by whether the community belongs to danwei or not. Danwei is a typical Chinese term denoting the Chinese socialist workplace and the specific range of practices that it embodies (Bray, Reference Bray2005). It could be the government department, public institution and enterprise (Feng et al., Reference Feng, Dijst, Wissink and Prillwitz2013). In the pre-reform era, danwei functioned as a cellular multifunctional work unit, integrating both productive activities and social life. Since the implementation of housing reform, although productive activities have been gradually separated from social life in those danwei communities, housing and supporting facilities in gated residential blocks are still maintained. In addition, compared to other types of community, danwei communities usually accommodate a greater number of co-workers and their families.
Open space within a community
Open space within a community indicates whether there is open space for physical activities and social interactions of residents within a community or not. In addition to describing the outside environment, this indicator represents the surroundings within a community.
Socio-economic status
Income
Income was measured based on the total earnings of the respondents, including wages or pensions, profits from investments and maintenance from children. The indicator was classified into two categories based on the average income of the respondents in the survey: (1) below 4,000 RMB per month and (2) 4,000 RMB per month and above.
Education
The education of respondents was assessed by the highest education level obtained. Since college-level education is an important divide, education attainment was categorised as: (1) below college-level education and (2) college-level education and above.
Living status
The living status of respondents was measured based on one question in the survey, ‘Do you live with your children?’, thus including two categories: (1) co-reside with children and (2) do not co-reside with children. Co-residence with children is an important feature of the laopiao, and this living pattern reflects the traditional Chinese culture influenced by Confucianism, in which the family is the basic unit of society. Under the roof of one family, parents foster children and children care for their parents (Fei, Reference Fei1983).
Results
Descriptive statistics
The description of the sample is shown in Table 2. Chi-square and t-tests are employed to compare the summary statistics between the local elderly people and the laopiao. Different patterns between the two groups were identified. Compared to the local elderly people, the laopiao tend to be younger, married and female. That is probably because younger elderly females are more helpful in looking after children and grandchildren. According to the survey, a larger share of the laopiao came from the countryside or less-developed urban areas outside Nanjing. It could partly explain why a higher proportion of the laopiao have lower levels of earnings and education attainments than their local counterparts. One significant feature of the laopiao is their living arrangement. As indicated by Table 2, the vast majority of the laopiao co-resided with their children (91.16%), whereas only half of the local elderly people chose this option (47.09%).
Table 2. Descriptive statistics
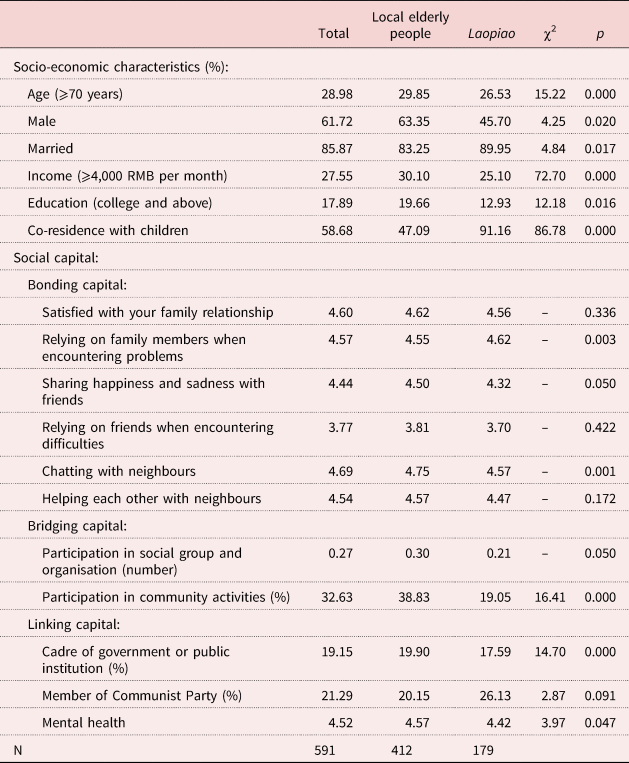
Concerning social capital, the disparity between local elderly people and the laopiao is apparent. Concerning bonding social capital, the laopiao are inclined to rely on personal networks (family members and friends) when encountering difficulties, while the social interactions with neighbours are significantly fewer than among the local elderly people. In terms of bridging social capital, the laopiao seem to have less heterogeneous social capital than their local counterparts, as they are less likely to participate in social groups, organisations or local community activities. It is somewhat revealing that the laopiao do not establish social networks in a new environment after leaving their hometowns. A larger share of local elderly people are/were the cadres of government or public institutions than among the laopiao, indicating that the local elderly people are more likely to be in a high position in urban China.
As expected, the laopiao reported a significantly lower level of psychological wellbeing than the local elderly people. In the following section, the underlying mechanisms of mental health between the two groups of elderly people are investigated and compared.
Structural equation modelling
Tables 3–6 show the standardised models as estimated by AMOS (version 17.0), which present the relationships among social capital, built environment and mental health of the local elderly people and the laopiao. The goodness-of-fit index is acceptable at 0.951 and 0.923, respectively (closer to 1), the root mean square error of approximation is acceptable at 0.043 and 0.049, respectively (less than 0.08), and the standardised root mean square residual is acceptable at 0.041 and 0.044, respectively (less than 0.08), indicating a good fit within accepted levels. In addition, we conducted a two-group analysis via Smart PLS (version 3.0) to compare statistically the differences of the associations between the local elderly people and the laopiao (shown in Table 7). As indicated by the tables, social capital and built environment significantly contribute to the mental health of elderly people. Nevertheless, different patterns of the relationships were observed between the local elderly people and the laopiao.
Table 3. Standardised coefficients of the structural equations model (local elderly people)

Significance levels : *p < 0.05, **p < 0.01, ***p < 0.001.
Table 4. Total effects of socio-economic status, built environment and social capital on the mental health of the local elderly people
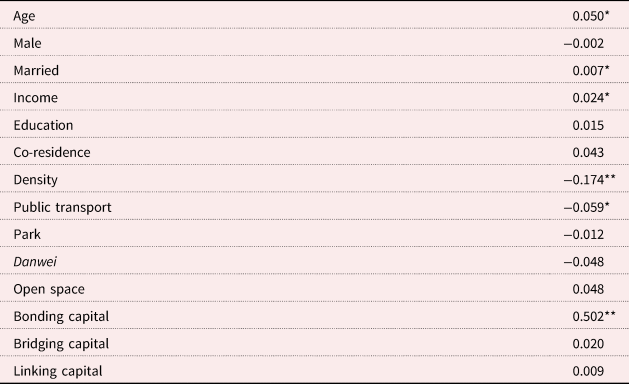
Significance levels: *p < 0.05, **p < 0.01.
Table 5. Standardised coefficients of the structural equations model (laopiao)

Significance levels: *p < 0.05, **p < 0.01, ***p < 0.001.
Table 6. Total effects of socio-economic status, built environment and social capital on the mental health of laopiao
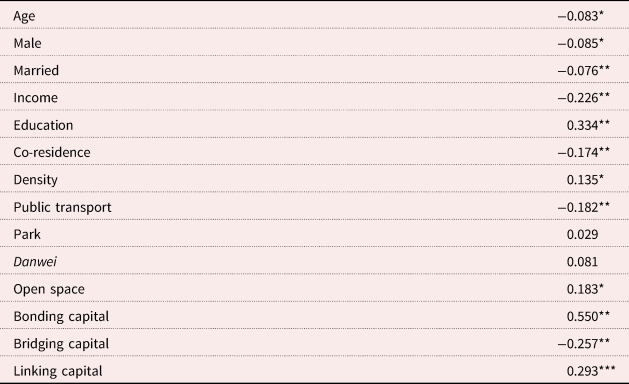
Significance levels: *p < 0.05, **p < 0.01, ***p < 0.001.
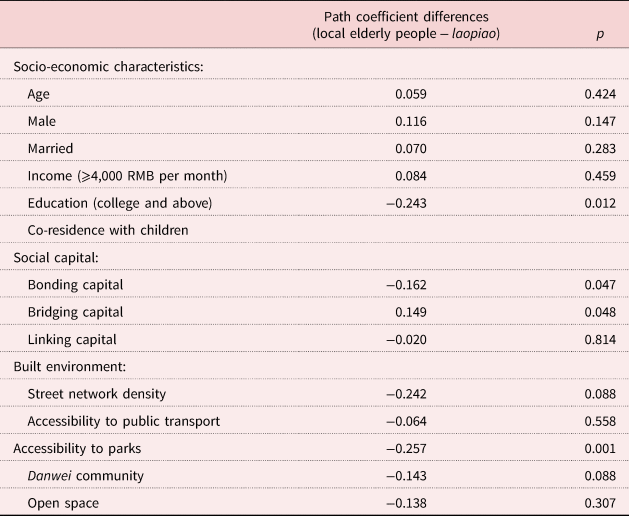
Table 7. Two-group analysis for mental health between the local elderly people and the laopiao
Social capital
Regarding social capital, there is a significant correlation between more bonding social capital and better mental health for the local elderly people and the laopiao, indicating the emotional support from personal networks has a positive effect on psychological wellbeing among elderly people in the Chinese context. Among the local elderly people, bridging social capital and linking social capital do not have a significant effect on mental health. In contrast, bridging social capital is negatively associated with the mental health of the laopiao, while the laopiao with more linking social capital reported better emotional health. This probably supports the conclusion that the laopiao, who float away from their familiar social environments and cut off their networks in their hometowns, experience poorer mental health. Nevertheless, evidence shows that elite elderly people can receive more material resources, respect and social trust than powerless people (Sundquist and Yang, Reference Sundquist and Yang2007; Norstrand and Xu, Reference Norstrand and Xu2012), which helps to maintain their privileges and expands guanxi in Chinese society. Compared to the mental health of the local elderly people, mental health among the laopiao is associated with more bonding capital but less bridging capital (see Table 7). The findings indicate that narrow social networks (i.e. family members, neighbours and friends) are more important for the laopiao to maintain their emotional wellbeing in an unacquainted surrounding, whereas the local elderly people, who usually have wider social networks, have a stronger need for social organisations and community activities. For both groups, access to heterogeneous rather than homogenous networks is more imperative, as people tend to receive more information and ideas through weak ties than through strong ties (Murayama et al., Reference Murayama, Nishi, Matsuo, Nofuji, Shimizu, Taniguchi, Fujiwara and Shinkai2013).
Significant correlations were found between observed variables and latent indicators representing the three dimensions of social capital. Nevertheless, the magnitudes of the effect estimates are different between the local elderly people and the laopiao. As indicated by Tables 2 and 4, the relationships with family members seem to be important for the bonding social capital of the laopiao. In terms of bridging social capital, for the local elderly people, the magnitude of participation in community activities is much greater than the magnitude of participation in social groups and organisations, while for the laopiao the magnitude of participation is similar for both. The laopiao, like floaters, are more prone to rely on personal networks (such as family members and friends) than on interpersonal relationships and they are more likely to isolate themselves from the local community.
Built environment
Among the local elderly people, street network density and distance to a park are significantly associated with mental health. The effects of the two indicators on mental health are negative, revealing that a sparser street pattern and closer proximity to greenspace promote the psychological wellbeing of the local elderly people. Escaping from crowded neighbourhoods may benefit the mental wellbeing of the local elderly people. In contrast, street network density has a positive significant effect on the mental health of the laopiao, probably because high-density street networks are usually found in old districts, where the laopiao mainly reside. In those districts, facilities such as shops, markets and restaurants are packed together, which is convenient for the laopiao to maintain their daily lives, enhancing their mental wellbeing. As shown in Table 7, living closer to a park is associated with better mental health among the local elderly people than the laopiao. Parks provide the local elderly people with outdoor open spaces for social interactions and physical activities, improving their psychological wellbeing (Sugiyama and Thompson, Reference Sugiyama and Thompson2007). The positive effect of the park on mental health of the laopiao is weaker, probably because they have fewer chances for outdoor activities in parks.
Distance to the metro station is negatively related to mental health for both the local elderly people and the laopiao. This finding indicates the significance of public transport access to physical activities and social interactions of elderly people, improving their mental wellbeing. Nevertheless, the presence of open space within the community only exhibits a statistically positive effect on the mental health of the laopiao. Compared to their local counterparts, the main job of the laopiao is to look after their children and grandchildren. Hence, their chance for outdoor recreation in parks is largely reduced. Open space within the community thus becomes an important place for them to interact with other neighbours, benefiting their mental health.
Socio-economic factors
Apart from the direct impact on mental health, socio-economic factors affect mental health through mediating with social capital and the built environment. Tables 3 and 5 present the total effects of covariates on mental health. Table 7 shows the differences in the effects of socio-economic factors on mental health between the local elderly people and the laopiao.
Among the locals, being older, married and higher-paid is associated with higher levels of mental health, which echoes prior research findings (Yip et al., Reference Yip, Subramanian, Mitchell, Lee, Wang and Kawachi2007). Nevertheless, the effects of those indicators are the opposite for the laopiao. That may be caused by the fact that the laopiao leave their hometowns and encounter many personal challenges in a new environment, e.g. getting older outside their hometowns, living separately from their husbands/wives, and so on. In addition, co-residence with children has a negatively significant effect on the mental health of the laopiao, hinting at the possible discomfort in the home of children. This may be attributable to the substantial value differences between generations in contemporary China. With the rapid changes of family structure in recent decades, the traditional social foundation such as filial piety has been weakened, resulting in depression among elderly people (Lim et al., Reference Lim, Chang, Yu, Chiu, Chong and Kua2011). Moreover, the lack of private space and time further reduces the level of mental health among the laopiao. Compared to the local elderly people, high education has a greater positive impact on the mental health of the laopiao. The finding indicates the importance of educational level in social interaction and communication, which can help the laopiao familiarise themselves with the new environment.
Conclusion
In recent decades, migration has dramatically changed the socio-economic landscape of contemporary China. The process is not only characterised by massive rural-to-urban migration, but it is also accompanied by the drastic increase in the laopiao in urban China. Basing our survey in Nanjing (N = 591), we investigate the association between social capital, built environment and mental wellbeing for elderly people in the Chinese setting. Our findings can help improve our understanding of the underlying mechanism through which social capital and the built environment affect the mental health of the local elderly people and the laopiao in urban China. Also, our findings provide hints for policy makers to adjust the existing policies to cater to the different groups of elderly people in urban China.
For the first research question, our findings demonstrate that the different dimensions of social capital have different effects on mental health among elderly people in the Chinese setting. Specifically, bonding social capital in terms of the relationship between family members, friends and neighbours positively associates with emotional wellbeing for both the local elderly people and the laopiao; whereas bridging social capital and linking social capital are only related to mental health among the laopiao. The findings indicate that Chinese elderly people rely heavily on ‘inward-looking’ social networks to maintain their mental wellbeing. First, in traditional Chinese culture that is based on the Confucian ideology, the family is regarded as the basic unit of society (Fei, Reference Fei1983). Despite the significant changes in Chinese society over a century, the traditional value of ‘family is important in people's life’ persists (Sun and Wang, Reference Sun and Wang2010). Such a belief is more prevalent among elderly people than among the youth, thereby affecting their health outcomes more significantly. Second, guanxi has been entrenched in Chinese society. Trust and social accommodation, which are observed to enhance mental wellbeing among elderly people (Forsman et al., Reference Forsman, Nyqvist and Wahlbeck2011; Ramlagan et al., Reference Ramlagan, Peltzer and Phaswana-Mafuya2013), are created among familiar persons through the reciprocity of favours in the Chinese setting (Tsui and Farh, Reference Tsui and Farh1997). Third, organisation-based social capital functions well in western countries, while it may not be the same in China. Chinese, especially elderly people, tend to depend on personal social networks rather than the members of organisations. Another plausible explanation is that the control of the non-governmental organisations by the Chinese government somewhat hinders the function of the organisation-based social capital among elderly people (Norstrand and Xu, Reference Norstrand and Xu2012).
In terms of the association between the built environment and mental health, we found a positive relationship between accessibility to subway stations and mental health among elderly people, which is in line with previous studies (Melis et al., Reference Melis, Gelormino, Marra, Ferracin and Costa2015). Public transport enables elderly people to access a wider variety of physical activities and social interactions, and narrows the gap by offering opportunities to reach needed facilities and services, benefiting mental health (Melis et al., Reference Melis, Gelormino, Marra, Ferracin and Costa2015). In recent decades, Chinese cities have expanded dramatically. In those large cities, the subway has become an essential means to link different parts of urban areas together. Compared to western countries, the percentage of elderly people who have driving licences is much lower in China. Hence, elderly people rely more on public transport (e.g. subway) than on private vehicles for outdoor activities. This further strengthens the importance of public transport to the emotional wellbeing of elderly people in urban China.
For the second research question, this study finds some differences between the local elderly people and the laopiao regarding the inter-relationship among social capital, the built environment and mental health. Concerning the association between social capital and mental health, ‘inward-looking’ social capital has a strong causal relationship to emotional wellbeing among the laopiao. Nonetheless, in contrast to the local elderly people, bridging social capital has a weaker effect on the mental health of the laopiao, while linking social capital has a stronger effect on the mental health of the laopiao. The findings imply that their floating status may influence the underlying mechanism of mental health among elderly people in urban China. Laopiao move from their hometowns to a new environment. Hence, strong relations with family members, friends and neighbours can help the laopiao adapt to new lives, although the sense of belonging to a community or neighbourhood, which is positively associated with wellbeing among elderly people (Young et al., Reference Young, Russell and Powers2004), needs time to be cultivated. Also, because the laopiao must look after their children and grandchildren, they have less time to participate in local organisations and community activities and, hence, they have weaker social integration and attachment. Laopiao are more dependent on emotional support from personal social networks, especially kinship networks. On the other hand, they tend to emphasise the significance of power-related linking social capital to enhance their mental wellbeing. In China, elite elderly people not only bring in more material resources but also receive more respect and wider guanxi through their connection. The privileged laopiao have more linking social capital helping them buffer the disadvantaged conditions in cities far from their hometown, thereby enhancing their emotional wellbeing; while for the powerless group, their inadequate linking social capital may lead to poor mental health. In other words, linking social capital may magnify the differences in mental wellbeing among the laopiao.
In terms of the association between the built environment and mental health, our findings reveal that the local elderly people and the laopiao may have different expectations towards the built environment, which relates to mental health. First, a lower density of street network contributes to better mental health among the local elderly people, while the association is the opposite for the laopiao. Higher street network density often facilitates better access to facilities and walkability. But, it is also associated with crowded and noisy living conditions. Earlier studies show that access to facilities and services can help improve mental health (Evans, Reference Evans2003). Yet, it is also reported that crowding may reduce the wellbeing of residents (Rodgers, Reference Rodgers1982). Facilities, especially retail, may attract outsiders and generate stress (Halpern, Reference Halpern1995). Compared to western countries, such adverse effects will be more apparent in China where the density of street networks and the population are already very high. Furthermore, the local elderly people and the laopiao may have different concerns in their daily lives. For instance, the local elderly people expect a quiet and spacious living environment, while the laopiao want convenience and social contact, which are essential for the emotional wellbeing of these new urban dwellers. Second, previous research states that open space encourages social interaction and physical activity, which has a positive relationship with people's mental health (Sugiyama and Thompson, Reference Sugiyama and Thompson2007). Given the limited mobility of elderly people, space near a residence has a greater effect on their wellbeing (Takano et al., Reference Takano, Nakamura and Watanabe2002). In this study, we found that access to a park has a greater effect on mental health among the local elderly people, while open space within a community is a significant mental health determinant for the laopiao. Although the association between access to green/open spaces and mental health has been widely conceived, our results indicate that the influences of different types of green/open spaces on mental health are different among different groups of elderly people.
Our findings come with some implications for elder care in urban China at the community level. First, in addition to family support and friendship, more community programmes are required to network the laopiao with the locals, which could help increase the place attachment and facilitate social exchange for the laopiao. Improved bridging social capital could help the laopiao to reduce their heavy reliance on personal social networks and connections with the elite. Second, instead of treating all elderly people as a homogenous group, policy makers should consider providing diverse built environments for different groups of elderly people. Compared to the commercial housing communities built after the housing reform, the old neighbourhoods in cities such as those danwei communities often lack open space. Therefore, besides constructing large-sized parks, open spaces such as greenery along streets and small parks should be scattered in residential districts to improve the mental wellbeing among various groups of elderly people. Third, the vast number of laopiao who look after their children and grandchildren may somehow reduce the number of nurseries in urban China. As a countermeasure, more nurseries should be provided to let those working families have other alternatives for taking care of their children. To conclude, this study shows that the mechanisms through which social capital and built environment affect mental health are heterogeneous among elderly people. Diversified policies are required to enhance the mental health of different groups of elderly people in urban China.
Financial support
This work was supported by the National Natural Science Foundation of China (41871135); and the Humanities and Social Sciences Foundation of the Ministry of Education of China (19YJCZH146).
Ethical approval
This project was reviewed and approved by Nanjing University (reference number 41871135).









