Introduction
Gerontology research has established that social relations improve or buffer health and increase life expectancies, although specific findings have been inconsistent (e.g. Berkman and Syme Reference Berkman and Syme1979; Russell and Cutrona Reference Russell and Cutrona1991; Ryff and Singer Reference Ryff and Singer2000; Seeman Reference Seeman2000; Sugisawa, Liang and Liu Reference Sugisawa, Liang and Liu1994). These inconsistencies may be due in part to the fact that most researchers have focused on the effects of isolated aspects of social relationships on mental and physical wellbeing (e.g. Avlund et al. Reference Avlund, Lund, Holstein, Due, Sakari-Rantala and Heikkinen2004; Larson, Mannell and Zuzanek Reference Larson, Mannell and Zuzanek1986). Such a variable-centred approach is valuable and informative, but in reality, individuals are embedded in social networks with arrays of attributes, such as small network size, frequent contacts with family, or considerable emotional support (Antonucci and Akiyama Reference Antonucci and Akiyama1987; Bosworth and Schaie Reference Bosworth and Schaie1997; Magai et al. Reference Magai, Consedine, King and Gillespie2003). It may be more informative to take a pattern-centred approach by examining types of social network profiles and their mental and physical health implications. Such a pattern-centred approach has been used to examine many aspects of heterotypical functioning among older adults, including cognitive, personality, physical and social functioning (Magai et al. Reference Magai, Consedine, King and Gillespie2003; Maxson, Berg and McClearn Reference Maxson, Berg and McClearn1997; Smith and Baltes Reference Smith and Baltes1997), and it may be particularly appropriate for examining the dynamic nature of social relations; for example, such dynamics are reflected in the various reasons for network loss combined with growing dependencies on others, and the conflict between the desires for closeness and autonomy.
Previous research on social network types has focused primarily on the structural aspects of social networks, such as network size and frequency of contacts (Bosworth and Schaie Reference Bosworth and Schaie1997; Litwin Reference Litwin1995, Reference Litwin2001; Litwin and Landau Reference Litwin and Landau2000; Melkas and Jylhä Reference Melkas, Jylhä and Litwin1996; Stone and Rosenthal Reference Stone, Rosenthal and Litwin1996; Takahashi, Tamura and Tokoro Reference Takahashi, Tamura and Tokoro1997; Wenger Reference Wenger1997). Across these studies, several relatively robust structural network types can be identified that are associated specifically with wellbeing: a diverse or diffuse network type (generally with the highest wellbeing), a restricted or socially-isolated network type (generally with the lowest wellbeing), a friend- and/or community-focused network type, and a family-focused network type. Prominent models and theories of social relations, such as the ‘theory of functional specificity’ (Weiss Reference Weiss and Rubin1974) and the ‘convoy model of social relations’ (Kahn and Antonucci Reference Kahn, Antonucci, Baltes and Brim1980) emphasise, however, the importance of the structure and function of social networks. For instance, according to ‘functional specificity theory’, relationships tend to become specialised in terms of the functions they serve, so that individuals require a number of different relationships to maintain wellbeing. According to the convoy model, in addition to the structure and function of social relations, the qualitative evaluations of individuals' social relations are fundamental to understanding their mental and physical health.
Most studies that have examined network types have been conducted in Europe and Israel. Their definitions of social network types and methods of network analysis have varied greatly, making it difficult to draw firm conclusions about network types, their health implications, and their universality. The present study attempts to address these gaps in the literature by including a variety of social relations characteristics (structural, functional, and qualitative) in the specification of network profiles, and by conducting parallel analyses in two countries, the United States and Japan.
For several reasons, it is particularly informative to compare social relations among older adults in Japan and the United States. First, both countries are experiencing population ageing, although Japan is ageing faster (Japanese Ministry of Internal Affairs and Communications 2004; US Census Bureau 2003), bringing issues associated with older adults (in particular, declining health and care-giving) to the forefront. Given the association of social networks with formal-care utilisation (e.g. Litwin Reference Litwin2004), it is important to understand better the universality or cultural-specificity of the attributes of older people's social networks and how they are differentially associated with mental and physical health. Secondly, although the two countries are economically similar, their historical, demographic, political and cultural differences make them prime candidates for comparison (Okabayashi et al. Reference Okabayashi, Liang, Krause, Akiyama and Sugisawa2004; Rothbaum et al. Reference Rothbaum, Pott, Azuma, Mikaye and Weisz2000). Thirdly, although recent research calls this simple dichotomy into question (e.g. Miller Reference Miller2002; Takahashi et al. Reference Takahashi, Ohara, Antonucci and Akiyama2002), the US and Japan are prototypical examples of what researchers have traditionally referred to as, respectively, ‘independent/individualistic’ and ‘interdependent/collectivistic’ cultures (Lansford Reference Lansford2004). In addition to the individualism/collectivism dichotomy, some researchers have also explained the cultural differences between the two countries in terms of the differences between equality (in the US) and hierarchy (in Japan) (e.g. Triandis Reference Triandis2001).
As a result of these cultural differences, the experience of social relations for older people in the United States and Japan may have clear contrasts. For example, for historical and geographic reasons, Japan is ethnically and linguistically relatively homogeneous. Although the image of Japan as completely mono-ethnic is a myth (Lie Reference Lie2001), 99 per cent of the population is Japanese and there are fewer than 1.5 million non-Japanese residents (Central Intelligence Agency 2006). Such homogeneity could impact upon social relations because of the larger base of shared linguistic and cultural values (e.g. different criteria for friendship). Furthermore, although individuals in both samples lived through World War II, Japanese older adults are more likely to have been personally affected by the war since their country experienced widespread and unprecedentedly severe enemy attacks.
In addition, partly in consequence of the longer life expectancies and the relative infrequency of divorce in Japan, older Japanese people are more likely to be married than older Americans (Japanese Ministry of Internal Affairs and Communications 2004; US Census Bureau 2003). In fact, among those aged 65 to 74 years, about 75 per cent of American men and 52 per cent of American women are married, compared to respectively 87 and 77 per cent among Japanese men and women. Furthermore, Japanese elders express a stronger preference for living with their children than do American older people (Sugisawa et al. Reference Sugisawa, Shibata, Hougham, Sugihara and Liang2002). The ‘stem-family-structure’ (i.e. elders living together with the oldest son, his wife and their grandchildren) is also much more common in Japan. As a result, social support for Japanese older people tends to be centred on the family more than the equivalent support systems in America (Koyano et al. Reference Koyano, Hashimoto, Fukawa, Shibata and Gunji1994; Takahashi et al. Reference Takahashi, Ohara, Antonucci and Akiyama2002). Although co-residence with children in Japan has declined during the past few decades as a result of several macro-demographic and social trends (Izuhara Reference Izuhara2004; Okabayashi et al. Reference Okabayashi, Liang, Krause, Akiyama and Sugisawa2004), co-residence and financial exchange with children is still much more common in Japan than in the United States. As a result, older Japanese people rely less on spouses, friends and neighbours than on their co-resident children.
In addition to these objective differences in social relations, the cultural meanings ascribed to social relations may differ between Japan and the United States. Some researchers believe that these differences stem from the overarching philosophical distinction between collectivism and individualism (Kitayama, Markus and Kurokawa Reference Kitayama, Markus and Kurokawa2000; Markus and Kitayama Reference Markus and Kitayama1991). In Japan, relationships are considered focal and objective. The major cultural task for the Japanese is to fit in and adjust to relationships while constraining personal desires. In contrast, in the United States, group ties are governed less by group norms, and Americans may be more willing to rely on or trust unfamiliar others (Rothbaum et al. Reference Rothbaum, Pott, Azuma, Mikaye and Weisz2000). More generally, there may be a tendency for relationships to be seen as voluntary in cultures such as the American, and as predetermined in cultures like the Japanese (Adams, Anderson and Adonu Reference Adams, Anderson, Adonu, Mashek and Aron2004). At the same time, recent comparative work has shown Americans to be more trusting and accepting than the Japanese of both friends and family, suggesting that the individualism/collectivism dichotomy must be treated as a heuristic descriptor rather than a theory for explaining Japanese/US cultural differences (Takahashi et al. Reference Takahashi, Ohara, Antonucci and Akiyama2002).
Furthermore, intimacy with one's spouse seems to have deeper cultural roots in societies that emphasise equality, such as the US, than in societies that emphasise hierarchy, like Japan (Palmore and Maeda Reference Palmore and Maeda1985; Triandis Reference Triandis2001), which suggests that very different meanings are ascribed to the role of spouse in the US and Japan. Indeed, unlike American husbands and wives, Japanese husbands and wives tend to have separate spheres of life, and communication gaps are both common and widely accepted (Sugimoto Reference Sugimoto and Sugimoto1997). Interestingly, although links between having a spouse and psychological and physical wellbeing have consistently been found in the United States (e.g. Berkman and Syme Reference Berkman and Syme1979; Kiecolt-Glaser and Newton Reference Kiecolt-Glaser and Newton2001), the comparable findings in Japan have been inconsistent (Sugisawa et al. Reference Sugisawa, Shibata, Hougham, Sugihara and Liang2002). Overall, these different cultural traits imply that types of social networks in the US and Japan differ, that similar social networks have different meanings for the Americans and the Japanese, and that different network types differentially associate with wellbeing.
In this paper we adopt the view of Miller (Reference Miller1999, Reference Miller2002) and other cultural researchers that culture and context are inextricably linked. Rather than assuming a simple dichotomy between the individualistic and the collectivistic, such a view requires recognising the ‘heterogeneity and overlap that exists between and within different cultural communities’ (Miller Reference Miller2002: 104) by making multi-dimensional comparisons across cultures (Takahashi et al. Reference Takahashi, Ohara, Antonucci and Akiyama2002). In this study, to allow for heterogeneity between and within the United States and Japan, we take a pattern-centred approach and conduct analyses separately by country. In forming our hypotheses and interpreting the findings, we acknowledge not only the influence of context on social relations, but also the possibility that contrasting cultural meanings are accorded to social relations.
Two main research questions, based on the previously reviewed research and speculations, have guided this study. First, what profiles of social relations (including their structural, functional and qualitative aspects) are typically found among older adults, and are these similar or different in the United States and Japan? To our knowledge no previous research has been conducted on multi-dimensional (i.e. structural, functional and qualitative) network types among older people. The analyses in the present study are therefore primarily exploratory. Given that previous research has established the robustness of particular structural network types (seeLitwin Reference Litwin1995, Reference Litwin2001; Litwin and Landau Reference Litwin and Landau2000; Melkas and Jylhä Reference Melkas, Jylhä and Litwin1996; Wenger Reference Wenger1997), it was hypothesised that a diverse network, a family-focused network, a friend-focused network, and a restricted network would emerge in one or both countries, but also that because of cultural differences in social relations, differences would also emerge.
The second research question is whether these network types are associated with mental and physical health when controlling for various background variables, and do these associations vary by country? Because network-type research and Weiss's (Reference Weiss and Rubin1974) ‘theory of the functional specificity of relationships’ imply that having diverse people in one's network brings better health than having a very restricted network, it was hypothesised that, in both countries, individuals in the most diverse networks would have better mental and physical health than those that had the most restricted networks. Although specific hypotheses regarding cultural similarities or differences were not developed, it was thought that differences might emerge as a result, for example, in the importance of the family as a source of social support among Japanese older people (Koyano et al. Reference Kiecolt-Glaser and Newton1994). It is important to note that because of the cross-sectional design, any associations between network types and health cannot be interpreted causally. Because mortality data were available, however, it was possible to examine for the US the variations in this outcome for the different social network types. It was hypothesised that, controlling for other known predictors of mortality, i.e. age, gender, education, race, and morbidity, individuals in the most diverse networks would have the highest likelihood of survival for 12 years.
Methods
The design and the participants
The US and Japanese data were drawn from the Social Relations and Mental Health over the Life Course Study (Antonucci and Akiyama Reference Antonucci, Akiyama, Nestmann and Hurrelmann1994). The analysis reported here is the first to use this data set to examine social network types. The first wave of data collection was undertaken during 1991 to 1993 by the University of Michigan Survey Research Center and by Central Research Services of Tokyo, using face-to-face interviews that lasted approximately 60 minutes. A probability sample stratified by age and gender was compiled to obtain regionally representative samples in the Detroit (N=1,702) and Yokohama (N=1,842) metropolitan areas. Adults aged 60 or more years were over-sampled, and only this age group was included in the present analysis. The American sample comprised 514 adults aged 60 to 93 years (41% men, 59% women), and the Japanese sample 491 adults aged 60 to 92 years (51% men, 49% women).Footnote 1 For the US data only, a mortality status assessment was obtained in September 2005 (about 12 years after the first wave of data collection).
Measures
Social network characteristics
In both countries, the characteristics of the respondents' social networks were assessed through the network mapping procedure developed by Antonucci (Reference Antonucci1986), by which an individual's network members are placed concentrically in three circles depending on feelings of closeness. The respondents were first asked questions about the structural characteristics of the first 10 people that they listed in their network, and then further questioned about the supportiveness of various close relationships. Relationships with spouse, closest child and same-sex best friend were included in the creation of the functional variables.
The structural variables included marital status (‘0’ for ‘not married’ and ‘1’ for ‘married’), total network size (number of people mentioned), proximity of the network (proportion of the network living within one hour's drive), frequency of contact with family members (‘0’ for none mentioned, and then an ordinal scale from ‘1’=‘irregularly/never’ to ‘5’=‘everyday’, averaged across all family members among the first 10 people named), and frequency of contact with friends (similarly calculated). The functional variables included the proportion of the network members in the inner circle (viz. the proportion of ‘close others’), a measure of instrumental support (created by averaging responses across the three relationships to two prompt sentences referring to financial help and sick care), and a measure of emotional support (created by averaging responses across the spouse, closest child and same-sex best friend to six prompt sentences using a five-category agree-disagree scale).Footnote 2 The qualitative variable was a measure of ‘negative quality’ created by averaging responses to two prompt sentences: ‘[Other] gets on my nerves’, and ‘[Other] makes too many demands on me'.
Socio-demographic variables
Age in years was a continuous variable, and gender a dichotomy (‘1’=male, ‘2’=female). Education level was a continuous variable of years of formal education (1 to 17+). Race, applied only to the US dataset, was established from a dichotomous variable (‘1’=Black, ‘2’=non-Black).
Outcome variables
For both data sets, depressive symptoms were measured by the 20-item Center for Epidemiologic Studies Depression Scale, the CES-D (Radloff Reference Radloff1977). The items ask how often during the last week the respondents had experienced a series of affective, somatic and inter-personal symptoms of depression. These are coded on a four-point Likert scale, from ‘1’ for ‘rarely/none of the time’, to ‘4’ for ‘most/all of the time’. Typically, the item scores ranged from ‘0’ to ‘3’, and a composite total was created by taking their sum, with a possible range from ‘0’ to ‘60’. As a result of excessive missing data in the Japanese dataset, however, a mean composite was created for both countries.Footnote 3 In both data sets, morbidity was represented by an index of the respondent's global subjective rating of his or her present health, which ranges from ‘1’ (excellent) to ‘5’ (poor), and by a count of chronic illnesses (e.g. heart trouble, problem with liver, stomach and/or intestinal trouble).
Results
Profiles of the social network clusters
To address the first research question about the typical profiles of social relations, separate cluster analyses were conducted in each country. Extreme outliers were eliminated, i.e. 10 from the US sample, to leave an analysis sample of 504 respondents, and 19 from the Japan sample to leave 472. All variables were standardised to t scores to eliminate scale difference effects (Hair and Black Reference Hair, Black, Grimm and Yarnold2000). Two clustering techniques (hierarchical and k means) were used, as in previous gerontological research (see Smith and Baltes Reference Smith and Baltes1997). Based on an examination of the multiple criteria available in Ward's SAS software procedures (pseudo-F statistic, pseudo-t 2 statistic, and Sarle's cubic clustering criterion), the appropriate number of clusters was confirmed for each country before the k-means iterative partitioning procedure was performed (procedure FASTCLUS in the SAS software). The hierarchical cluster analysis statistics indicated that the best solution for the US data had six clusters, whereas the best solution in Japan had five clusters. The final k-means cluster analyses provided respectively the best six- and five-cluster solutions. Table 1 provides the names of the common and country-specific network types, as well as their prevalence and general descriptions. Tables 2 and 3 present the specific cluster solutions for the United States and for Japan.
TABLE 1. Names, prevalence and descriptions of older people's network types in the United States and Japan, 1991–93

TABLE 2. Group means or proportions for the nine social relations variables by network type in order of prevalence, United States

Notes: N=504. Mean counts and proportions are reported on both the original scale and as standardised to an overall mean of 50 and a standard deviation of 10. Because many of the original scores can be interpreted as percentages, all are given with two decimals (but note the possibility of spurious accuracy). Bold numbers indicate defining peaks of the profiles (specifically, approximately 0.5 or >0.5 standard deviations above or below the sample mean).
TABLE 3. Group means or proportions for the nine social relations variables by network type in order of prevalence, Japan

Note: N=472. Mean counts and proportions are reported on both the original scale and as standardised to an overall mean of 50 and a standard deviation of 10. Because many of the original scores can be interpreted as percentages, all are given to two decimals (but note the possibility of spurious accuracy). Bold numbers indicate defining peaks of the profiles (specifically, approximately 0.5 or >0.5 s.d. above or below the sample mean).
As shown in Table 1, most of the network types that emerged in both countries corresponded to the four network types commonly found in the literature: diverse, friend-focused, family-focused, and restricted. We refer to these as the ‘common network types’. For each country, however, the number and composition of the more specific network types under each of these categories varied; we therefore gave these types more specific names that refer to their structural, functional and qualitative differences. We refer to these as the ‘country-specific network types’. In both the United States and Japan the analysis identified a diverse network type. The diverse/extensive network type in the US (the most prevalent type: 32%) comprised mostly married individuals with large networks (on average almost 11 people), and reported above-average levels of support and a below-average frequency of negative relations. The diverse/supported network type in Japan was less prevalent (17%) and comprised primarily married people who reported frequent contact with friends, much emotional support, and a network predominanted by geographically-proximate individuals (83% lived close by).
In Japan there was one friend-focused network type and in the US there were two. A generally positively-supported friend-focused network type accounted for 22 per cent of the US networks and 20 per cent of the Japanese. In the US, the friend-focused/supported network members were primarily unmarried, had frequent contact with friends, and reported above-average levels of instrumental and emotional support. In Japan, the members were all unmarried, had large networks, frequent contact with friends, a relatively small proportion of close others, and average levels of support. In the US, a friend-focused/unsupported network type also emerged (11%), whose members were also likely to be unmarried. Although they also reported frequent contact with friends, they reported low levels of instrumental and emotional support and a small proportion of close others.
In both countries there was a family-focused network type. In the US, only 10 per cent of the sample fell into a family-focused/negative network type. Individuals in this network type reported small networks and that about 90 per cent of the members lived within one hour's drive, and they rated 88 per cent of them as ‘very close’. They reported above-average frequency of contact with family but below-average frequency of contact with friends. Most interestingly, they rated their relationships as highly negative. In Japan, a family-focused/close network type (the most prevalent type: 29%) had both married (n=84) and widowed (n=45) individuals with relatively small embedded networks; that is, frequent contacts with family, very irregular contacts with friends, and a large proportion (95%) of close others.
In Japan there was one restricted network type and in the US there were two. The structurally-restricted network type (17% prevalence) in the US was ‘restricted’ primarily in the structural social-relations variables. The unmarried individuals in this network type seemed neutrally disconnected, in that they reported having a below-average proportion of proximate network members and being in contact with friends very irregularly, but also reported relatively low levels of negativity. The functionally-restricted network type in the US (8%, the lowest prevalence), on the other hand, was restricted primarily in terms of its functions. The informants reported low levels of instrumental and emotional support from its members and rated the relationships as highly negative. In Japan, individuals in the restricted/unsupported network type (10%, the lowest prevalence) reported relatively small local networks with 72 per cent of the members proximate. This network type was also functionally restricted; the predominantly married individuals in this network type reported receiving very little positive support. As with the structurally-restricted network type in the US, however, individuals in this network type reported relatively low levels of negative relations. Finally, in Japan there was a unique married and distal network type (24% prevalence) that comprised exclusively married individuals whose network members tended not to live close by (only about 27 per cent of the network members lived within one hour's drive). They also reported having a relatively small proportion of close others (38%).
Differences by network types in socio-demographic variables
The associations between the socio-demographic variables and the network types established from the cluster analyses were examined as a test of the criterion validity of the cluster solution. Variables not used to form the clusters but suspected of varying across clusters (i.e. the background variables) were used to test for cluster differentiation (Hair and Black Reference Hair, Black, Grimm and Yarnold2000). For the dichotomous background variables (gender and, in the US, race), chi-squared analyses were performed. For the continuous background variables (age and education), one-way analyses of variance were performed with the cluster type as the independent variable. Post-hoc Tukey pairwise comparisons were performed in order to examine the bivariate associations.
In both the United States and Japan, the social network types differed in terms of gender, age and educational attributes (and in the US, in prevalence by race) (see Table 4), confirming the cluster differentiation (Hair and Black Reference Hair, Black, Grimm and Yarnold2000). In both countries, the friend-focused network types included mostly women, whereas the diverse network types each had a narrow majority of men. In the US, the youngest (average age just under 69 years) and most educated individuals were in the diverse/extensive network type. In Japan, although the youngest individuals were in the restricted/unsupported network type and the most educated in the married/distal network type, individuals in the diverse/supported network type did not differ significantly from those in either of these other network types in terms of age or education. In Japan the oldest (just under 74 years) and the least-educated individuals were in the friend-focused network type, whereas in the US the oldest individuals (average age almost 75 years) were in the structurally restricted type, and the least-educated individuals were in the family-focused/negative networks. Furthermore, in the US the largest percentage of Black Americans was in the family-focused/negative network type.
TABLE 4. Age, education, gender (and race) by network type in the United States and Japan

Notes: 1. For continuous variables, means in the same column that do not share subscripts differ at p<0.05 in the Tukey comparison.
Significance levels: ** p<0.01, *** p<0.001.
Wellbeing by network type
Multivariate analyses of co-variance were conducted to examine the associations of the network types with depressive symptoms and morbidity simultaneously, controlling for age, gender, race (in the US), and education. For the US, the multivariate significance of the network type was established (Wilks' Λ=0.94, F (degrees of freedom (df) 10, 986)=2.95, p=0.001).Footnote 4 The univariate analyses revealed a significant difference across network types for depressive symptoms (F (df 5, 390)=4.17, p=0.001), with a trend towards a significant difference for morbidity (F (df 5, 554)=2.12, p=0.06). Post-hoc comparisons using the Bonferroni correction (see Table 5) revealed that individuals in the functionally-restricted network type had the highest levels of depressive symptomology, which was significantly higher than for those in all other network types except the family-focused/negative network type. Those in the functionally-restricted network type also reported the lowest levels of physical health, which was significantly worse than for those in the family-focused/negative network type.
TABLE 5. Estimated standardised means (in t-scores), controlling for age, education, gender (and race) for the US and Japan

Notes: 1. Means in the same column that do not share subscripts differ at p<0.05 in the Bonferroni comparison. No significant differences were found in Japan.
2. Higher scores indicate worse physical health, so that both estimated means (depressive symptoms and morbidity) can be interpreted in the same direction.
By contrast, in Japan, the network cluster types were not significantly associated with depressive symptoms or morbidity. Multivariate significance for network type was not present (Wilks' Λ=0.99, F (df 8, 926)=0.77, p=0.63). The estimated means for depressive symptomotology and morbidity, controlling for age, gender, and education, are shown in Table 5 for each network type.
Survival by network type
Mortality in the sample was available at the time of writing only for the US. By September of 2005, 258 of the original 504 had died. Among the deceased participants, the average interval between the first data collection or Time 1 and death was 7.4 years (standard deviation=3.6). The dates of the deaths of nine deceased participants were unavailable, so they were omitted from this analysis. The deceased individuals were significantly older, less educated and had more chronic illnesses at Time 1 compared to the survivors. There was no significant gender difference between the survivors and the deceased, but the deceased were more likely to be non-white. Cox regression models were used to relate the network types at baseline to mortality, since these models can take censored cases into account (Cox Reference Cox1972). By entering the variables in blocks, the effect of network type beyond that predicted by background variables could be determined (using a chi-squared change test from Block 1 to Block 2). Specifically, the predictor variables age, gender, race, education and count of chronic illnesses at Time 1 were added in the first block, and dummy codes representing the network types (with the functionally restricted type as the reference category) were added in the second block.
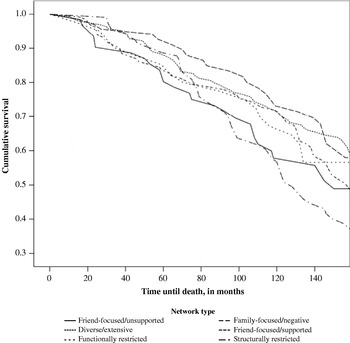
As can be seen in Table 6, older individuals, males and those with a greater number of chronic illnesses at Time 1 were at an increased risk of death during the follow-up interval. Although the addition of the network types in the second block contributed to this model only at the level of a trend (χ2 (df 5)=10.5, p=0.062), one significant pairwise comparison was identified: the mortality hazard for individuals in the structurally restricted network type was 1.44 times that of those in the functionally restricted networks. Figure 1 presents the survival functions separately for each network type at the mean of the covariates. It shows that whereas those in the ‘diverse/extensive’ network type had the highest probability of survival, those in the structurally restricted type had the lowest.

Figure 1. Survival functions for the US sample 1991–2005, controlling for covariates.
TABLE 6. Results from Cox regression analyses predicting mortality status in 2005

Notes: Diverse/extensive, friend/supported, structurally restricted, friend/unsupported, and family/negative represent dummy-codes for these network types; the functionally restricted network type is omitted from the analysis as the comparison group.
Significance levels: ** p<0.01, *** p<0.001.
Discussion
This study has expanded the social relations and network-type literature using an approach that is consistent with major theories of social relations (e.g. Antonucci Reference Antonucci, Binstock and George1990; Kahn and Antonucci Reference Kahn, Antonucci, Baltes and Brim1980; Weiss Reference Weiss and Rubin1974). We have examined the diversity of multiple relationships and their varying functions and quality in the United States and in Japan. The findings suggest that there are common network types that are quite robustly identified across different cultures and that are consistent with previous social network typologies (e.g. Fiori, Antonucci and Cortina Reference Fiori, Antonucci and Cortina2006; Litwin Reference Litwin2001; Litwin and Landau Reference Litwin and Landau2000; Wenger Reference Wenger1997). In both countries, at least one ‘diverse’, one ‘restricted’, one ‘friend-focused’, and one ‘family-focused’ network type were identified. In addition, the analysis has confirmed the existence of culturally-specific network types and of cultural differences in the composition and prevalence of certain network types, as well as their associations with mental and physical health. For example, whereas in the United States individuals in the functionally restricted network type had the highest levels of depressive symptoms and morbidity and the lowest life satisfaction, there were no differences in wellbeing by network type in Japan. Although only cross-sectional correlations have been shown, it was additionally found that the US network types had implications for survival.
Number, composition and prevalence of network types
The inclusion of all aspects of social relations (i.e. structural, functional, and qualitative characteristics) in the taxonomy of network types allowed a more nuanced assessment of individuals' social networks than has been achieved by previous research on structural variation in social network types. Consistent with such research, in both the United States and Japan, we found five to six different network types. This implies that adding functional and qualitative variables does not greatly multiply the number of identified types of social networks, but rather indicates that certain structures associate with certain functions, as ‘functional specificity theory’ predicts (Weiss Reference Weiss and Rubin1974). For instance, individuals in diverse networks tend to receive a great deal of instrumental and emotional support and to be fairly satisfied with their networks. Some findings from the present study, however, indicate that structure and function do not always correlate. For example, as predicted, we found that some network types are primarily distinguished by functional characteristics (e.g. the US functionally restricted network type), and also that network types with similar structures have different functions (e.g. the two US friend-focused network types). We also found two types of restricted network types: those restricted primarily in structure (e.g. the US structurally restricted type), and those restricted primarily in function (e.g. the US functionally restricted type and the restricted/unsupported type in Japan). These findings highlight the importance of the simultaneous examination of structure and function.
Further evidence for the distinctiveness of structure, function and quality lies in the cultural differences found in their associations. For example, unlike in Japan, Americans in family-focused networks rated their relationships as particularly negative compared to those in other network types, in spite of relatively high levels of received support. It could be that frequent contact with and close proximity to family members can lead to emotionally intense relationships, which may be both more affectionate and more distressing (Lüscher and Pillemer Reference Lüscher and Pillemer1998; Willson, Shuey and Elder Reference Willson, Shuey and Elder2003). In Japan, by contrast, family-focused networks were not distinguished by high levels of negativity. This may be because of the high value placed on family (Koyano et al. Reference Koyano, Hashimoto, Fukawa, Shibata and Gunji1994; Takahashi et al. Reference Takahashi, Ohara, Antonucci and Akiyama2002), the lower levels of intimacy between husbands and wives (Sugimoto Reference Sugimoto and Sugimoto1997), or the unacceptability of admitting publicly that there are negative aspects of an intimate relationship. Interestingly, negative relations did not distinguish any of the Japanese network types from each other, implying that there is little variation in negative personal relationships in Japan, or at least little variation in the readiness to describe them. Consistent with this possibility is the smaller standard deviation in negative relations in Japan (0.83) than in the US (0.94).
We also found differences by country in the prevalence of several common or shared network types. For instance, whereas the diverse network type (diverse/extensive) was most prevalent in the US, it was relatively uncommon in Japan. The low prevalence in Japan seems to imply that such diverse networks among married individuals are less valued or normative in that society than networks focused more on the family (Koyano et al. Reference Koyano, Hashimoto, Fukawa, Shibata and Gunji1994). In contrast, the prevalence of the family-focused network type in the US was quite low, whereas it was the most prevalent in Japan. This is not surprising, given the high value placed on family in Japan, the typical ‘stem-family-structure’ living arrangements, and the evidence that the Japanese are more likely than Americans to name family members as the most important people in their networks (Koyano et al. Reference Koyano, Hashimoto, Fukawa, Shibata and Gunji1994; Takahashi et al. Reference Takahashi, Ohara, Antonucci and Akiyama2002).
The married and distal network type in Japan was unique to that country and distinguished by a small proportion (27%) of the network living proximally; in addition, individuals in this network type were all married and had a relatively small proportion of close others in their networks. The identification of this network type in Japan could be a sampling artefact. For instance, the tendency for Japanese husbands and wives to have separate spheres of life may be more problematic for older people in urban than rural settings, because rural networks generally enable a wider range of interactions with relatives and neighbours (Sugimoto Reference Sugimoto and Sugimoto1997). Because the Japanese data in the present study were drawn from a large city (Yokohama), it may be that married individuals whose networks were peripheral had difficulty maintaining close relationships with others. On the other hand, the fact that the married/distal network type was exclusive to Japan may be because intimacy with one's spouse has deeper cultural roots in societies that emphasise equality, like the US, than in societies that emphasise hierarchy, like Japan (Palmore and Maeda Reference Palmore and Maeda1985). Marital relations in the United States tend to be based on affective bonds, whereas in Japan they are primarily role-based. It may be that in other countries, such as the US, being married plays more of an integrating function in the lives of older adults in general. This possibility is supported by the finding that the network type with the largest proportion of married individuals in the US was in the married and extensive type (a diverse type), in which network size and levels of support are both high, whereas in Japan it was in the married and distal type.
Socio-demographic differences by network type
In light of the cultural similarities and differences in the compositions and prevalence of the network types, the socio-demographic characteristics of individuals in the different network types are of considerable interest. For instance, the Japanese individuals in the unique married/distal network type tended to be highly-educated men. This may relate to the fact that older Japanese men (aged 60 or more years) are more likely than older Japanese women to be married (above 80 years-of-age, more than three times more likely) (Japanese Ministry of Internal Affairs and Communications 2004). Furthermore, highly-educated older Japanese men may maintain more peripheral networks. According to the third author, a native of Japan, the married/distal network type is the typical social network of retired Japanese men in urban areas. Many have moved to the city for their jobs, commuted long distances and worked long hours so that they have virtually no connections in the community. Upon retirement, these men lose their work-related social networks and have only their spouse remaining.
Consistent with previous research on structural social-network types (e.g. Fiori, Antonucci and Cortina Reference Fiori, Antonucci and Cortina2006; Litwin Reference Litwin2001), the youngest, most-educated individuals tended to be in the most diverse networks, and the oldest, least-educated individuals tended to be in the most restricted. Interestingly, however, individuals in the functionally restricted network types were relatively young compared to those in the other network types. This is consistent with evidence that younger people tend to be more negative about their social relations than older people (Birditt and Fingerman Reference Birditt and Fingerman2003). In fact, in Japan the youngest individuals were in the restricted/unsupported network type (primarily a ‘functionally-restricted’ network type). These findings demonstrate that although structurally restricted networks may be most common among the oldest-old, functionally restricted networks are not limited to the oldest-old. Another interesting exception to this trend is the relatively older age of those in the friend-focused network types in both countries. In fact, those in this type in Japan had the highest average age. Given that in both countries, the friend-focused network types consisted mainly of unmarried women (as found previously, seeFiori, Antonucci and Cortina Reference Fiori, Antonucci and Cortina2006; Litwin and Landau Reference Litwin and Landau2000), it is likely that these older women are turning to their friends for support after their spouses have died.
In the US, those with the lowest levels of education were in the family-focused/negative network type. This finding may represent a cultural anomaly that derived from the ethnic diversity of the US sample. Specifically, this was the most prevalent type among Black Americans, which is consistent with previous research that has shown that, in comparison to Whites, Black Americans tend to have smaller family-centred networks with whom they have more frequent contacts (Antonucci Reference Antonucci, Birren and Schaie2001). Two facts may drive this finding: (1) Black Americans have lower life expectancies than Whites, thereby reducing the number of peers available to be network members; and (2) historically repressed minorities have lower levels of education (a characteristic of those in the family-focused/negative network type).
Wellbeing differences by network type
One of the most surprising findings of the correlation analysis was the lack of any significant associations between wellbeing and network types in Japan, especially considering the importance that is customarily placed on relationships in Japan (Kitayama, Markus and Kurokawa Reference Kitayama, Markus and Kurokawa2000; Markus and Kitayama Reference Markus and Kitayama1991). Previous research has shown, however, a weaker association between social relations and wellbeing in Japan than in western cultures (e.g. Berkman and Syme Reference Berkman and Syme1979; Kiecolt-Glaser and Newton Reference Kiecolt-Glaser and Newton2001; Sugisawa et al. Reference Sugisawa, Shibata, Hougham, Sugihara and Liang2002). Furthermore, in their study of Australian and Japanese individuals aged 17–69 years, Schumaker et al. (Reference Schumaker, Shea, Monfries and Groth-Marnat1993) found a high inverse correlation between loneliness and life satisfaction among the Australian participants, but a much smaller inverse relationship among the Japanese participants.
There could be several reasons for this lack of association, some of which may stem from unique cultural or historical circumstances. As mentioned earlier, in comparison to many other affluent countries, Japan is relatively homogenous ethnically and linguistically. It may be that the lack of significant differences by network type reflects low variation in depression and morbidity. Supporting this hypothesis were the lower standard deviations for both depressive symptoms and number of chronic illnesses in Japan compared to the United States. On the other hand, the null finding in Japan may derive from a response bias that some believe is common among the Japanese, specifically that Japanese respondents tend to choose intermediate responses from Likert scales (e.g. Janevic et al. Reference Janevic, Ajrouch, Merline, Akiyama and Antonucci2000), perhaps because of a cultural disposition to disapprove of extreme opinions. Such response biases may limit the variation in the CES-D in the present study, thereby concealing actual differences.
Turning to an interest of cultural psychologists (Miller Reference Miller1999, Reference Miller2002), it is important to consider the possibility of differing meanings of the American and Japanese social-network types. Specifically, Japan's cultural norms of interpersonal harmony and unity encourage the accommodation of relationships while constraining individual desires (Kitayama, Markus and Kurokawa Reference Kitayama, Markus and Kurokawa2000; Markus and Kitayama Reference Markus and Kitayama1991; Triandis Reference Triandis2001), whereas in western societies, like the US, the ‘key to relational wellbeing may be the creation of intimate connections with large numbers of people as a safeguard against the experience of loneliness’ (Adams, Anderson and Adonu Reference Adams, Anderson, Adonu, Mashek and Aron2004: 330). Because in Japan relationships may be viewed as predetermined or obligatory, rather than constructed or voluntary, the Japanese may ‘learn’ to be happy with whatever network they have. In contrast, Americans may regard belonging to certain network types (e.g. restricted networks) as non-normative, especially since there may be a need to appear connected, appealing and romantically desirable (Rokach, Bacanli and Ramberan Reference Rokach, Bacanli and Ramberan2000), and because social networks may be viewed as constructed or voluntary. This implies that in the United States, social-network types are more likely to be associated with well-being.
In the US, although individuals in the functionally restricted network type had the highest level of depressive symptoms and the worst physical health (consistent with our predictions concerning ‘restricted’ network types), there was variation across the two types of wellbeing for the high-functioning network types. In particular, individuals in the family-focused/negative network type had relatively high levels of depressive symptoms but the fewest physical-health problems. It is possible that the close-knit, local family members of this network type are particularly attentive to an individual's physical health, e.g. ‘encouraging’ healthy behaviour and ‘reminding’ an older person about medical regimens. These ‘encouragements’ and ‘reminders’ may become highly negative relationship experiences. Furthermore, because friendship ties tend to be voluntary whereas ties with kin are obligatory (Antonucci and Akiyama Reference Antonucci, Akiyama, Blieszner and Bedford1995), belonging to a family-focused network type (especially in a society that values voluntary relationships) may have negative implications for mental health. Thus, close family relationships may simultaneously be associated with better physical health and worse mental health.
Survival by network type
The results of the survival analysis in the US imply that network types have causal implications for mortality. After controlling for age, gender, race, education, and number of chronic illnesses, individuals of the structurally restricted network type were at a greater risk of dying during the follow-up interval than those of the functionally restricted type. It could be that the mortality rate of those in the structurally restricted network type is being driven by their marital status, since being single or widowed has been found to predict mortality (e.g. Ho Reference Ho1991). Alternatively or additionally, the high mortality risk for those of the structurally restricted network type (compared to those of the functionally restricted type) may relate to the former's relative isolation. In other words, it may be that having unsupportive and negative relationships is better for longevity than having no relationships at all.
Limitations of the analysis
Several limitations of the present study should be acknowledged. First, given the nature of the samples, the generalisability of the findings is limited. More specifically, although one strength of the datasets is that they are community-based representative samples, in both countries they were collected from metropolitan areas (Detroit and Yokohama, respectively) during the early 1990s. Older adults' social networks tend to be smaller and to provide less support in urban than in rural areas (van Tilburg and van Groenou Reference van Tilburg and van Groenou2002); also, relations with extended kin tend to be looser, whereas those with friends and acquaintances tend to be more important (Höllinger and Haller Reference Höllinger and Haller1990). Furthermore, while it appears that some social network types are culture-bound, it is important to keep in mind that some may also be cohort-bound. However, the findings of the present study are fairly consistent with previous research on structural social-network types using larger, geographically-diverse samples from other birth cohorts (e.g. Litwin Reference Litwin2001; Melkas and Jylhä Reference Melkas, Jylhä and Litwin1996), which implies that certain findings may be generalisable.
Secondly, the primarily cross-sectional nature of the analyses limits the ability to draw causal conclusions (particularly with respect to the wellbeing outcomes). For instance, it cannot be assumed from this study that being in a diverse network type improves health; it could be that people who foster positive and supportive relationships or who are less depressed are also more likely than others to have varied, diverse networks. In fact, research has shown that distressed individuals may withdraw from or alienate social relationships (Matt and Dean Reference Matt and Dean1993), and that high levels of depression or physical limitations may actually lead to declines in emotional support over time (Gurung, Taylor and Seeman Reference Gurung, Taylor and Seeman2003). Given the likelihood that the association is bi-directional, it is still of interest that there was no association for the Japanese sample, and may herald the need for a deeper exploration of social relations in Japan. Furthermore, based on the significant mortality effects in the US, at least some causality in relation to the network types can be inferred.
Thirdly, some limitations in the variable definitions and measurement should be acknowledged. For instance, in calculating frequency of contacts, rather broad definitions of ‘family’ and ‘friend’ were used to minimise missing data. It is clear from the literature, however, that specific ties, such as sibling ties (Cicirelli Reference Cicirelli1989, Reference Cicirelli, Smith, Tobin, Roberston-Tchabo and Power1995), or peripheral ties such as co-workers and acquaintances (Fingerman Reference Fingerman, Lang and Fingerman2004), may have unique effects on wellbeing, and that different combinations of family and friend relationships (e.g. children, spouse and confidant) also have differential effects on wellbeing (Dean, Kolody and Wood Reference Dean, Kolody and Wood1990; Dykstra Reference Dykstra1990; Koropeckyj-Cox Reference Koropeckyj-Cox1998; Phillips et al. Reference Phillips, Bernard, Phillipson and Ogg2000; Pinquart Reference Pinquart2003; Simons Reference Simons1983–Reference Simons4). A related limitation is that because of missing data, separate measures for emotional and instrumental support from family compared to friends were not used. It was assumed that individuals in the US friend-focused and supported network type (labelled ‘friend-focused’ because of frequent contacts with friends) were receiving support primarily from friends. Because some types of support that are normally provided by kin may be less beneficial when provided by non-kin and vice versa (Felton and Berry Reference Felton and Berry1992), it may be important to examine different types of emotional and instrumental support separately by type of relationship. There is also evidence that the associations among different types of support from different relationships may be culture-bound. For example, Lansford (Reference Lansford2004) found that family relationship quality is more strongly related to friendship quality in Japan than in the United States. Finally, assessing the ‘quality’ of social relations using a quantitative approach presents difficulties, not the least of which is a tendency for such items to be positively skewed.
Conclusions and future research
In spite of these limitations, the analysis has provided evidence of the heterogeneity of older adults' social networks. By taking a pattern-centred rather than a variable-centred approach, and by including structural, functional and qualitative social-relations variables in the analyses, this study has assessed individuals' social relations and has addressed some of the inconsistencies and complexities in previous findings on social relations and health among older people. For instance, when studied out of context, negative relations tend to affect health negatively (e.g. Rook Reference Rook, Stephens, Crowther, Hobfoll and Tennenbaum1990), but the pattern-centred analyses have shown that experiencing low levels of relationship negativity in the context of an impoverished network (e.g. the structurally restricted network type in the US) may be worse for mortality than experiencing high levels of relationship negativity in a less isolated network (e.g. the US functionally restricted type). These findings are consistent with Seeman's (Reference Seeman1996) speculations that the inconsistencies in the epidemiological evidence on social relations and health may stem from a positive association between social integration and other more negative aspects of relationships.
Although this study suggests that there is a common network typology that is quite robust across different cultures, it also confirms the existence of culturally-specific network types and of cultural differences in the composition and prevalence of certain types, as well as in their implications for mental and physical health. It is important to acknowledge that the vulnerability of different groups of older people, or at least the expression of that vulnerability, may be culturally-specific. Those developing social policy must balance an understanding of cultural values with the varying needs of different groups of elders. For example, the ‘back-to-the-family’ policy of long-term care currently favoured in many western countries (Litwin Reference Litwin and Litwin1996) may be incongruous with the most dominant and/or most supportive network types in those countries.
The present study is but a first step in understanding the complexities of the types, functions and perceived quality of relationship networks. Future research can build upon the present study by creating typologies of more specific aspects of individuals' social relations (e.g. instrumental support from children, companionship from friends and/or a spouse) and that refer to personal, situational and contextual factors (e.g. personality, living arrangement, stressors). Furthermore, longitudinal research is needed to assess the causal link between social-network types and health, the developmental processes involved in network formation (Litwin Reference Litwin1995), as well as how and why older adults move into and out of certain network types. In sum, this study offers evidence for the theoretical and practical significance of network types in the field of social relations and health and in different countries.
Acknowledgements
The collection of the survey data was funded by the Ministry of Education in Japan (grant 02301016) to Hiroshi Azuma and his research group, and by grants from the US National Institute for Mental Health (MH46549-02) and the US National Institute on Aging (AG13490 01 A1) to Toni C. Antonucci and Hiroko Akiyama. The generous sources of support that made the present study possible included the University of California San Diego and the Summer Training on Aging Research Topics-Mental Health Fellowship; the National Science Foundation's East Asia and Pacific Summer Institute; the American Association of Retired Persons Scholarship; and the Daniel Katz Dissertation Fellowship. We gratefully acknowledge those in the Life Course Development Program at the University of Michigan for their useful comments.