


Introduction
Like many developed countries, Australia has a growing population of older people (Australian Institute of Health and Welfare (AIHW) 2007) who present with an increasing prevalence of chronic conditions, such as coronary heart disease and diabetes (Australian Bureau of Statistics (ABS) 2006). There are also concerns about the prevalence of inactivity among older people, given its impact on health and functional capacity. Physical activity is identified as an important protective factor in five of the Australian National Health Priorities, including: cardiovascular disease prevention, diabetes prevention and control, cancer prevention, injury prevention and control, and the promotion of mental health (AIHW 1997; Bauman et al. Reference Bauman, Bellew, Vita, Brown and Owen2002). In addition, physical activity is often prescribed in the management of chronic conditions. Current national guidelines recommend that all adults should do 30 minutes of moderate-intensity exercise on most, preferably all, days of the week (Commonwealth Department of Health and Aged Care 1999).
The Victorian Burden of Disease study (Vos and Begg Reference Vos and Begg1999: 28) attributed 7.3 per cent of the mortality burden in men and 9.3 per cent of that in women to physical inactivity, with three-quarters of the attributable burden occurring in people aged 65 or more years. Physical activity is the second most important area for risk factor reduction (after smoking) in older people with regard to the overall burden of disease (Bauman and Smith Reference Bauman and Smith2000). As expressed by Evans (Reference Evans1999: 12), ‘there is no segment of the population that can benefit more from exercise than the elderly’. The research evidence, however, shows that physical activity amongst older adults tends to decrease with age and that older women tend to be less physically active than older men (National Ageing Research Institute 2003). In Australia, only 51 per cent of men and 37 per cent of women aged between 60 and 75 years are classified as sufficiently active to attain health benefits from the activity (Armstrong, Bauman and Davies Reference Armstrong, Bauman and Davies2000).
Previous research in this area has explored how physical activity is influenced by various socio-demographic and psychosocial variables, such as gender, socio-economic status, physician advice, perceived exercise benefits, self-esteem, self-efficacy, motivation, childhood exercise, knowledge, health and injury (Li, Fisher and Brownson Reference Li, Fisher and Brownson2005; Schutzer and Graves Reference Schutzer and Graves2004). Education, social class and socio-economic indicators have been found to influence health behaviours across the lifespan and to be significant predictors of physical activity levels among older Australians (Kendig, Browning and Teshuva Reference Kendig, Browning and Teshuva1998). Cohen-Mansfield, Marx and Guralnik (Reference Cohen-Mansfield, Marx and Guralnik2003) also found health problems, lack of motivation, lack of time, fatigue, bad weather and not liking physical activity to be commonly reported barriers amongst community-dwelling older people; whereas motivators for exercise included feeling better, having someone to exercise with, and having an organised programme. In this study, women reported both a greater number of barriers as well as motivators than men.
A growing body of research is concerned with the impact of societal and structural factors on levels of physical activity. Gebel and colleagues identified 128 primary research studies between 1980 and 2005 that examined the relationship between physical activity and the environment (Gebel, Bauman and Petticrew Reference Gebel, Bauman and Petticrew2007). For older people in particular, environmental factors known to influence positively physical activity and health include: green and open spaces for recreation, number of street intersections, perceptions of safety, number of nearby recreational facilities (Li et al. Reference Li, Fisher and Brownson2005); having shops and other facilities within a ‘walkable’ distance (<20 minutes) (King et al. Reference King, Brach, Belle, Killingsworth, Fenton and Kriska2003); ‘neighbourhood walkability’ (Berke et al. Reference Berke, Gottlieb, Moudon and Larson2007); perceived presence of a mall and walking trail (Michael et al. Reference Michael, Beard, Dongseok, Farquhar and Carlson2006); a perception of good quality facilities in the area (social/leisure, facilities for older people, rubbish collection, health services, transport, closeness to shops, somewhere nice to walk), and high levels of neighbourliness (Bowling et al. Reference Bowling, Barber, Morris and Ebrahim2006). Perceptions of problems in the area (e.g. noise, crime, air quality, rubbish/litter, traffic and graffiti) were also found to be predictive of poorer health (Bowling et al. Reference Bowling, Barber, Morris and Ebrahim2006; Michael et al. Reference Michael, Beard, Dongseok, Farquhar and Carlson2006). In a rare longitudinal study, Dawson and colleagues found amongst older people attending ‘walking schemes’ that having a health problem which restricted walking exacerbated people's negative perceptions about external barriers to neighbourhood walking, and that these increased over 12 months (Dawson, Sundquist and Johansson Reference Dawson, Sundquist and Johansson2005).
For older people, physical activity constitutes a key intervention for both the prevention of the aforementioned diseases and to retain their capacity to undertake activities of daily living (Andrews Reference Andrews2002; Bauman and Smith Reference Bauman and Smith2000; World Health Organisation (WHO) 2006). In their review of physical activity interventions, Kahn et al. (Reference Kahn, Ramsey, Brownson, Heath, Howze, Powell, Stone, Rajab and Phaedra2002) found individually-adapted behaviour-change programmes to be effective; they also provided examples of informational interventions, social support in community settings and an environmental and policy intervention to illustrate the various options for promoting physical activity beyond the individual level. These interventions illustrate the ways in which social-psychological and health-education models have also been used to good effect. Living in a disadvantaged area is also known to have a negative impact on the level of physical activity (Kavanagh et al. Reference Kavanagh, Goller, King, Jolley, Crawford and Turrell2005). Forty per cent of adults who lived in the most disadvantaged socio-economic areas in Greater Melbourne were physically inactive, compared with 25 per cent in the least disadvantaged areas (ABS 2001).
A pronounced feature of the Australian population is its ethnic diversity, with more than 200 different cultural groups. In 2001, the overseas-born were estimated to be 33 per cent of the population (AIHW 2002). Of these, around one-third had migrated from English-speaking countries, while among the remainder there are large representations of people born in Greece, China, Poland, Italy, Malta, Vietnam and Macedonia. The Australian population of older people from culturally-diverse backgrounds currently accounts for approximately 18 per cent of the total in the age group, and is projected to increase to around 23 per cent by 2011 (Gibson et al. Reference Gibson, Braun, Behnam and Mason2001). In Australia, insufficient levels of physical activity have been shown to be more prevalent among culturally-diverse people born overseas than among the Australian-born (AIHW 2003). Specifically, 81.8 per cent of people born in Southern and Eastern Europe, and 79.5 per cent of people born in North Africa and the Middle East, exhibit sedentary or low exercise behaviours, as opposed to 69.2 per cent of the Australian-born (ABS 2006). Given that they are more sedentary, people from culturally-diverse populations are at greater risk of the adverse health consequences of physical inactivity (Wilcox et al. Reference Wilcox, Castro, King, Housemann and Brownson2000).
In the United States (USA), sedentary lifestyles have also been found more prevalent in culturally-diverse communities than in the general population (Mouton et al. Reference Mouton, Calmbach, Dhanda, Espino and Hazuda2000). Michael et al. (Reference Michael, Beard, Dongseok, Farquhar and Carlson2006) found, for example, that younger white people demonstrated higher levels of neighbourhood walking than older people and culturally-diverse groups. Given the country's distinct immigration patterns, however, findings from the USA and other continents may not be replicated in Australia. In Australia's multicultural society, some important lifestyle choices are influenced by the traditions and customs inherent in a particular cultural group, as well as by linguistic ability and ease of communicating in the dominant English language (Armstrong, Bauman and Davies Reference Armstrong, Bauman and Davies2000; Bauman et al. Reference Bauman, Bellew, Vita, Brown and Owen2002; Centre for Culture Ethnicity and Health 2006), but little systematic research has examined physical activity patterns in Australia's culturally-diverse communities (Centre for Culture Ethnicity and Health 2006). The pilot phase of the study reported here investigated the barriers to physical activity of older women from three different cultural groups. It found that Italian women were more likely than Anglo-Celtic women to report personal barriers, while Vietnamese women were more likely than Italian and Anglo-Celtic women to describe their physical environment as less safe for walking, less attractive and having more crime (Bird et al. Reference Bird, Kurowski, Feldman, Browning, Thomas, Seedsman and Lau2009). Despite some differences in reported barriers across cultural groups, no differences were observed in the levels of activity. In summary, older people from cultural minorities, particularly those living in disadvantaged areas, are known to be particularly at risk from chronic disease and to have lower activity levels, but there has been little systematic investigation of the relationship between levels of physical activity and ethnicity, with a view to increasing rates of physical activity participation (DiPietro Reference DiPietro2001).
Aims
To address this gap, the aim of this study was to investigate the facilitators and barriers to physical activity for older people from culturally-diverse communities in lower socio-economic status areas in the western suburbs of Melbourne (Migrant Resource Centre 2004). This research project was part-funded by the area's local government authorities (LGAs) to inform their future health and physical activity policies and strategies. The specific aims and objectives were:
1. To determine and compare the levels of physical activity across older people from different cultural groups;
2. To identify and compare the barriers preventing older people from different cultural groups from participating in physical activity; and
3. To determine the predictors of physical activity participation in a culturally-diverse group of older people.
Methods
Study setting and recruitment
The study was conducted in three local government areas in the western region of Melbourne, in the State of Victoria, one of the most multicultural regions in Australia. Based on ABS 2001 census data, the percentage of the population aged 60 or more years in these areas ranged from 7.2 to 18.2 per cent, and 17.2, 44.3 and 53.9 per cent of people in the study areas spoke languages other than English, as compared to 25.8 per cent in the Melbourne Statistical Division. Older people were recruited through local community groups and Home and Community Care services, and the groups identified by the local authorities as being the most populous groups in the area were targeted: Anglo-Celtic, Croatian, Greek, Italian, Macedonian, Maltese and Vietnamese. Further details regarding the recruitment strategy employed, as well as a critical analysis of the challenges of recruitment, have been reported elsewhere (Feldman et al. Reference Feldman, Radermacher, Bird, Browning and Thomas2008).
The questionnaire
A survey questionnaire was constructed using items from four established instruments:
1. The St Louis Scale: ‘Measuring Physical Activity in Communities’ (Brownson et al. Reference Brownson, Chang, Eyler and Ainsworth2004). This instrument assesses the degree to which certain factors prevent people from exercising. It asks about walking, safety, what people like or dislike about the places where they walk, community, personal and social factors. Items are based on a five-point Likert scale, from ‘1’ (never prevents from exercising) to ‘5’ (very often).
2. The Neighbourhood Environment Walkability Scale (NEWS) (Saelens et al. Reference Saelens, Sallis, Black and Chen2003). This includes questions about streets and facilities within the neighbourhood, safety and perceptions of crime. Items are based on a four-point Likert scale, from ‘1’ (strongly disagree) to ‘4’ (strongly agree).
3. The International Physical Activity Questionnaire (IPAQ) (Craig et al. Reference Craig, Marshall, Sjostrom, Bauman, Booth, Ainsworth, Pratt, Ekelund, Yngve, Sallis and Oja2003). This records physical activity over seven days at three levels of intensity, namely walking, moderate and vigorous activity. Physical activity scores were weighted according to the IPAQ data processing guidelines to produce a metabolic equivalent score (MET) in minutes-per-week: walking or moderate intensity physical activity values were multiplied by one, and vigorous activity values by two. Scores of 150 or greater indicate the attainment of recommended levels of physical activity. In order to avoid errors from over-reporting, durations exceeding 28 hours (1,680 minutes) per week were truncated at 28 hours.
4. Self-reported health. This item was taken from the short form Health Survey Questionnaire (SF36). Perceived overall health during the last 12 months was rated on a five-point Likert scale from ‘1’ (poor health) to ‘5’ (excellent health).Footnote 1
Procedures
The questionnaire was written in English but administered in each participant's preferred language by multilingual interviewers at a location convenient to the participant. The interviewers had considerable and diverse experience of research and interviewing. All had worked in their own language communities (e.g. as professional translators and interpreters, community and welfare workers), and had a high level of English proficiency. They were chosen specifically for their ability to work in a dynamic translation environment. The multilingual interviewers were briefed about the aims and objectives of the study, and undertook training with the research team about interviewing older people, administering the questionnaire, and recording the quantitative data in English. Repeated contacts between the interviewers and the research team throughout the data collection process provided an opportunity to address any issues as they arose. Commonly, the interviews took place at a local cultural or community centre, or in the participant's home, and lasted on average 60 minutes.Footnote 2
The analyses
The data were initially analysed using descriptive statistics and the chi-squared test of differences between cultural groups and by sex. Differences between cultural groups were also analysed using Kruskal-Wallis tests. Non-parametric analyses were employed as the dependent variable, MET minutes per week, was not normally distributed. Associations between cultural group and activity level, and activity levels with barriers to physical activity, were investigated using chi-squared. Univariate analyses were used to explore significant factors for the regression analyses. Standard multivariate linear regression analyses were used to identify factors associated with participation in physical activity. Values for the sub-component levels of activity (walking, moderate and vigorous) were truncated at 180 minutes, as per the IPAQ guidelines and the total score was square-root transformed. A hierarchical regression analysis was conducted, using the enter method and three blocks of variables. Variables were chosen on the basis of their significance in the univariate analyses. The socio-demographic variables including self-rated health were entered into Model 1, neighbourhood variables into Model 2, and the St Louis variables into Model 3.
Results
The participants
Of the 408 older people who initially expressed an interest in participating and signed a consent form, 362 were interviewed. Of these, 29 were excluded from the analyses because they did not meet the inclusion criteria: 14 were too young, eight were not from the targeted cultural groups, six lived outside the designated local region, and one lived in a nursing home. Table 1 indicates that the age and gender distributions of the participants from the seven cultural groups were similar, as they were across the three LGAs (Melton had 22 per cent of the sample, Maribyrnong 35 per cent and Brimbank 43 per cent). The Anglo-Celtic participants reported living in Australia for longer (mean 61 years) than the other groups, with 62 per cent being born in Australia. In comparison, the Vietnamese participants had lived in Australia for the shortest time (17 years), and the means for the other five groups ranged from 34 to 48 years (Table 1). The Vietnamese also reported the shortest duration at their current address (105 months) and the lowest prevalence of full home ownership (20%), with 33 per cent being renters and 34 per cent living with their family, as in ‘their son's property’. One-quarter (27%) of the participants lived alone, with variation among the cultural groups being from zero (Macedonian) to 52 per cent (Anglo-Celtic). The majority (87%) lived in a house and were full owners (76%). The data on home ownership (76%) and reliance upon pension as main source of income (84%) suggest that many of the participants were ‘asset rich but income poor’.
Table 1. Socio-demographic profiles of the samples by cultural group

Notes: 1. The Anglo-Celtic group were older than all the others except the Croatians (p<0.05). The Macedonians were younger than all other groups except the Greeks (p<0.05). 2. The Anglo-Celtic group had been in Australia for significantly longer than the other groups (p<0.001). The Vietnamese had been in Australia for significantly less time than the other groups (p<0.001). 3. The Vietnamese group had been at their current address for significantly less time than the other groups (p<0.001). 4. The Vietnamese had significantly fewer reporting full home ownership (p<0.001). 5. Fewer Macedonians lived alone. 6. Fewer Anglos relied on the state pension as their main source of income. 7. Fewer Macedonians used local government home and community care services.
Physical activity
The most commonly reported forms of physical activity were: walking (83%), housework (men 24%, women 59%); gardening (men 46%, women 35%); and shopping (men 25%, women 37%). Recreational physical activity (e.g. tai chi, yoga, swimming, cycling, dancing, and bowling) and/or formal exercise (e.g. strengthening exercises, aerobics, exercise bike, and treadmill) were undertaken by around 20 per cent. The median duration of physical activity per week for the whole sample was 285 minutes (range of group means, 175–940). All gender by cultural-group subgroups except Macedonian women had a median score above the recommended minimum of 150 minutes per week (Table 2). There was, however, a vast range in the individual values from zero to the truncated maximum of 1,680 minutes. Overall, 66 per cent of participants reported attaining the recommended minimum of 150 minutes per week. This accords with the Australian physical activity guidelines recommended level to attain health benefits. This frequency did not differ between groups (range 55–75%; chi-squared p=0.34). People living alone were just as likely to attain more than 150 minutes of physical activity per week as those who lived with others (66% v 68%, p=0.79).
Table 2. Minutes per week of physical activity by gender and cultural groupFootnote 1

Notes: 1. Minutes per week of total physical activity were not normally distributed (Kolmogorov-Smirnov p<0.001), and therefore the non-parametric Kruskal Wallis test was used to compare cultural groups. 2. Difference of medians between men and women, p<0.005. 3. Differences of medians between groups, χ2, p=0.04. 4. Differences between groups, χ2, p=0.65. Differences between groups, χ2, p=0.34.
A two-way analysis of variance of gender by cultural group indicated that there was no difference between the reported amount of physical activity by men and women, or between the percentages of the two genders that attained 150 minutes per week, nor was there a group by gender interaction for minutes of exercise. A comparison between cultural groups revealed that the Italians reported far greater mean durations of physical activity than the other cultural groups (p<0.001), but they did not differ significantly in the percentage exceeding 150 minutes per week.Footnote 3
The sample was then ranked according to the reported minutes of activity per week and divided into tertiles (most active, intermediate durations, and least active). The ethnic composition of the three activity level tertiles significantly differed (χ2=48.5, p=0.00) (see Table 3). The most active tertile had a high proportion of Maltese (53%) and Italians (60%), and a small proportion of Macedonians (14%) and Croatians (17%). The numbers of participants were more evenly spread across cultural groups in the least active tertile.
Table 3. Distribution of participants in each cultural group by activity level tertile

Note: Chi-squared statistic (12 degrees of freedom), χ2=48.541, p=0.000.
Perceptions of neighbourhood
When assessing their area in terms of places available for walking, all groups recorded a favourable average (>2.5 on a scale of ‘1’ to ‘4’), the group means ranging from 2.8 to 3.1, and there were no statistically significant differences (F=1.94, p=0.08). There was, however, a significant difference in the perceptions of how aesthetically pleasing their area was for walking (F=8.33, p<0.001), with the Croatians (mean 2.3) perceiving their neighbourhood to be less aesthetically pleasing than virtually all of the other groups, and the Italians also reporting a lower score (2.6) than many of the groups (the range was from 2.3 to 3.0). There were also significant differences among the groups in their perceptions of neighbourhood safety and crime (F=5.02, p<0.001). The reported scores were reversed so that less than 2.5 is again a favourable score. The group mean scores ranged from 2.5 to 3.1, and groups tended to cluster; with the Greek (mean=3.1) and Anglo (mean 3.1) groups perceiving their neighbourhood to be most safe, the Macedonians (mean=2.5) as least safe, and the Italians (mean=2.8), Vietnamese (mean=2.8), Maltese (mean=2.8) and Croatian (mean=2.9) providing intermediate scores. There were no differences (F=0.05, p=1.00) between men and women in their perceptions of the availability of places to walk in their neighbourhood, neighbourhood aesthetics (F=2.63, p=0.07), or neighbourhood safety (F=0.72, p=0.29).
Barriers to physical activity
The prevalence of each barrier is reported in Tables 4 and 5. There was a high prevalence of personal issues across all the cultural groups, including: poor health, lack of energy, no motivation, and fear of injury. The data also indicated that the weather was frequently perceived to be a barrier, with a lack of a ‘safe place to exercise’ also of concern. There were differences in the mean number of barriers per person reported by the cultural groups. These differences were statistically significant, with the Anglo-Celtic (3.9) and Italian (4.3) groups reporting significantly (F=8.51, p<0.001) fewer barriers than the Macedonians (6.5) and Croatians (7.2). Women reported significantly more barriers than men (5.5 vs 4.7, F=5.93, p=0.02). Four barriers in particular were significantly more likely to be reported by women (Table 4): ‘I am not in good health’, ‘I don't have the energy to exercise’, ‘I am afraid of injury’, and ‘not having a safe place to exercise’.
Table 4. Percentage of respondents indicating that the specified barriers were experienced sometimes, often or very often

Table 5. Frequency of reporting specific barriers by cultural group
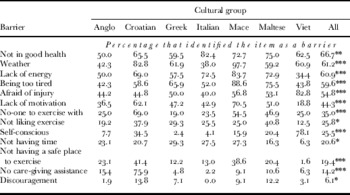
Significance levels: Differences among cultural groups *** p<0.001, ** p<0.01, * p<0.05.
When the specific barriers to physical activity were compared across cultural groups, several significant differences were identified (Table 5). Amongst these, the Vietnamese more frequently reported personal issues such as being more ‘self-conscious’ and being ‘afraid of injury’ as a barrier. Further investigation revealed that members of this group wished always ‘to look respectable’ in public, which had implications about what they would wear when going out. The Macedonian and Croatian participants were more likely to report bad weather, and not having a safe place to exercise, as barriers. The Macedonian group were also more likely to report physical capacity as a barrier, with a higher frequency reporting ‘lack of energy’, ‘too tired’, and ‘don't have the motivation’ as barriers. The Croatian participants' were more likely to report a lack of personal support, as indicated by the higher prevalence of: ‘having no one to exercise with’, and ‘having no care-giving assistance’. When the prevalence of barriers was compared across activity level tertiles, not surprisingly the ‘most active’ one-third reported fewer barriers per person (least active 6.3, intermediate active 4.7, and most active=3.6), and the differences were all statistically significant (p<0.01) (Table 6). When comparing the prevalence of specific barriers, the ‘least active’ had significantly greater prevalence for most of the barriers, but compared to the ‘intermediate active’ group, did not differ in prevalence of barriers related to being self-conscious, not having time, and being discouraged by others.
Table 6. A comparison of the barriers (St Louis Scale) by activity level tertile

Note: The p values are for the chi-squared statistic.
Predictors of activity
Linear regression analysis was conducted to identify the environmental predictors of physical activity behaviour in MET minutes per week. The regression models included the environmental, personal and social factors that contributed to physical activity among the participating groups. The final model explained 26 per cent of the variance in the dependent variable (Table 7). Reporting that footpaths were well maintained (beta −0.15, p=0.00) and that trees give shade for footpaths (beta −0.15, p<0.01) were negatively associated with physical activity. Interestingly, those perceiving their environment positively were less likely to be active, whilst those who were more active were not necessarily rating their neighbourhood positively. Whilst the Neighbourhood Environment Walkability Scale assesses neighbourhood walkability, its relationship to participants' behaviour is not simple. As expected, those reporting fear of injury, not having a safe place to exercise and poor health as barriers were less likely to be active.
Table 7. Predictors of MET-minutes per week of physical activity

Model statistics: Model 1: F (4,278 degrees of freedom)=6.95*** adjusted R 2=0.08; R 2 change=0.09***. Model 2: F (7,275 df)=5.45*** adjusted R 2=0.10; R 2 change=0.03*. Model 3: F (11,271 df)=10.06*** adjusted R 2=0.26; R 2 change=0.17***.
Note: CI: confidence interval.
Significance levels: * p<0.05, ** p<0.01, *** p<0.001.
Discussion
Concerning the first aim of this study, older people reported a wide range of physical activity levels, with the Italian and Maltese being the most active, and the Macedonians and Croatians least active. There were no differences in the reported levels of physical activity between men and women. These findings do not seem to concord with the literature that reports a higher prevalence of inactivity in culturally-diverse groups, particularly among women. With regard to the second aim of the study, the majority of barriers to physical activity were common across all cultural groups. Many of these barriers were personal, such as perceived health and lack of motivation, which supports Cohen-Mansfield and colleagues (Reference Cohen-Mansfield, Marx and Guralnik2003) findings for community-dwelling older people. Such barriers present a major challenge to the implementation of service deliverers' and government agencies' strategies for increasing physical activity. In particular, the barriers relating to perceived poor health and fears of injury may establish a downward spiral, with a failure to exercise at the recommended levels reducing health and physical capacity further. There may, however, be some scope to tackle the barriers relating to lack of motivation and fear of injury through psychological and behavioural interventions.
The barriers of ‘lack of time’ and ‘lack of care-giving assistance’ suggest the need for additional support services. Although it was interesting to note that a ‘lack of time’ was also reported with a similar frequency whatever the level of activity, the more active may have strategies for overcoming this barrier, or indeed give physical activity a higher priority. ‘Bad weather’ as a barrier can clearly be addressed through the provision of indoor facilities, but for this to be viable, access and transport to the location, as well as the cost to the participant need to be considered. Location of activities was an issue also raised in Lewis et al.'s study where Indo-Chinese participants reported liking outdoor activities, while Jewish participants preferred to be active indoors (Lewis et al. Reference Lewis, Szabo, Weiner, McCall and Piterman1997). As a means of ensuring opportunities for indoor activity, one participating local council in our study has since established walking groups in the local shopping mall.
As part of the research process the bilingual interviewers kept in regular contact with the university-based research co-ordinator. Through this channel, the team were able to gain another perspective regarding the levels of, and barriers to, physical activity of participants. Of note is a comment from an Italian interviewer who explained that the majority of Italian immigrants had come to Australia after World War II and they worked very hard and had no time for leisure activities. She emphasised that for these immigrants, having now retired, physical activity is not part of their routine or lifestyle so it was unlikely that they would be active, or have the inclination to be so. Likewise, a Maltese interviewer noted that it was not in the nature of older Maltese people to play sport or be physically active: ‘they may walk to the shops and play bingo, but that is the extent of it’. In the context of this study, however, Maltese and Italian groups actually reported relatively high levels of physical activity. This was predominantly in the form of domestic duties, while the interviewer's comments may have related more to leisure-based activities. This observation indicates that the migrant experience may be a key influence on type and amount of physical activity, and should be an avenue for further research.
The same Maltese interviewer also referred to the critical importance of transportation for Maltese women. Maltese women generally do not drive, and rely heavily on their husbands for transport. If their husbands die, then they can become very physically and socially isolated. This is not only because they cannot get to places but because they are often uncomfortable being unaccompanied. This example highlights the importance of investigating and being aware of specific cultural norms and the impacts they may have on physical activity behaviour.
Clearly, while barriers to activity were reported across all cultural groups, there were some differences in their relative frequencies. A qualitative study by Lewis et al. (Reference Lewis, Szabo, Weiner, McCall and Piterman1997) also found that barriers to activity varied cross-culturally within an older population. Interestingly, these researchers also emphasised the enormous individual variation in each cultural group, found that some exercise modalities are culturally specific (e.g. Tai Chi for the Indo-Chinese), and identified different cultural conceptualisations of exercise itself, which confirm our own findings. Furthermore, this current study found differences in the frequency of barriers reported according to activity tertile and gender. This indicates that while it is essential to acknowledge the influence of cultural experience on physical activity patterns, it may represent only one aspect of an intricate web of factors.
With regard to the built environment, all cultural groups reported a favourable score in their perceptions of neighbourhood safety and crime, but in comparison to the other studied groups, the Italians and the Macedonians had the lowest scores. Considering that the Italians were one of the most active groups, and the Macedonians the least active, it appears that perceptions of neighbourhood safety and crime did not uniformly influence activity levels in this study. This is confirmed by the neighbourhood safety and crime items not being identified as predictors of physical activity. Of course, the Italians, being more active, may have had more exposure and awareness of crime in the area. So, while perceptions of the neighbourhood may not have been wholly associated with levels of, or barriers to, physical activity it does not negate the influence of the environment. Future studies may help to identify cultural differences in activity levels according to objective indicators (e.g. Geographic Information Systems). Kavanagh and colleagues' (Reference Kavanagh, Goller, King, Jolley, Crawford and Turrell2005) study clearly indicated that low socio-economic areas are not as conducive to activity as less disadvantaged areas. Replicating such a study with greater numbers of older people from diverse cultural backgrounds, for example, may provide further insight. Clearly, the potential for environmental factors (such as the provision of paved and shaded footpaths that are separated from the traffic, recreation areas that enable social interaction and increased number of local facilities) to be addressed through public planning policies makes this an obvious target for research.
The third aim of the study sought to determine the predictors of physical activity participation. Neighbourhood walkability was negatively associated with physical activity behaviour. This could suggest that activity is taken outside the local area, or in spite of sub-optimal surroundings. The participants confirmed that perceived poor health can act as a barrier to physical activity uptake. Those who perceived fear of injury and having no safe place to exercise as barriers were less likely to be active. The importance of perception of safety has clear implications for the role of local government in supporting the development of safer communities or, at least, of the perception that they are safe. Unfortunately, the small sample sizes of some of the cultural groups made it impossible to compare the predictors of physical activity according to ethnicity. This is certainly an issue that demands further investigation in future studies.
Conclusions
This study has made an important contribution to a topic that lacks substantial research evidence, which can be partly attributed to the difficulties of conducting research among older people from different cultural groups (Feldman et al. Reference Feldman, Radermacher, Bird, Browning and Thomas2008). The main difficulties include accessing culturally-diverse communities, and the recruitment of both participants and bilingual and appropriately skilled interviewers. Flexible and creative approaches to recruitment are required, which is inconsistent with using a standard procedure across groups. A further limitation of this study was that the budget did not allow for the questionnaire to be translated and back-translated into each community language.
Another issue that needs to be addressed in such studies concerns the different cultural meanings attributed to the terms ‘exercise’ and ‘activity’. Having conducted a few interviews, one of the Greek interviewers noted that the concept of exercise was problematic and not easily understood by the participants. Indeed, the data indicate that while about one-half of the Greek participants said that they did housework, only 10 per cent regarded this as a form of activity which contributed to their scores on the International Physical Activity Questionnaire. The same applied to the Vietnamese participants, while the Italians, Maltese and Anglo participants were much more likely to report housework as a moderate activity. Of course, this pattern may have been partly because some interviewers' encouraged the participants to report housekeeping as an activity. Lewis et al. (Reference Lewis, Szabo, Weiner, McCall and Piterman1997) also found discrepancies in what did and did not constitute exercise. They found, for example, that Italians defined exercise as a ‘deliberate’ activity while housework was considered to be part of the lifestyle, in contrast to the Jewish and Greek groups that did consider housework to be exercise. This highlights the need for more research into cultural conceptualisations of physical activity and exercise, the implications for measuring levels of physical activity, and for the design of interventions to promote more activity. Another important feature of this study was the local focus. Nationwide studies that investigate physical activity patterns often cannot account for the nuances of the local area. By working closely with three local government authorities, the researchers were able to ensure that the findings of the research could be used to inform policy and practice directly in each specific area.
In summary, this study has indicated that while there may be some cultural differences in the levels of and barriers to physical activity, these differences are not always clear cut. Indeed, there may be a complex interaction of factors that influences activity levels and barriers, including cultural background, gender, service needs, age, neighbourhood, health, and perceptions. Thus, cultural identity is just one of several factors that need to be taken into account in programmes that seek to increase levels of physical activity amongst older people. We therefore endorse the recommendation of Lewis et al. (Reference Lewis, Szabo, Weiner, McCall and Piterman1997) that older people from culturally-diverse communities should be involved in planning, marketing and implementing any exercise and other health promotion efforts. This involvement should also extend to planning and policy development at the local government level.







